
Voice AI for Emergency Departments — Surge Intake & Human-First Escalation Support

Provincial and state health systems face unique pressures: centralized booking backlogs, seasonal surges, policy-driven intake rules, and public accountability. Off-the-shelf IVR tools rarely meet governance, privacy, and procurement expectations.
Peak Demand delivers fully managed, custom-built Voice AI deployments for public sector health environments across Canada, with U.S. alignment where applicable. Workflows are designed to support policy-aligned routing, least-privilege integration, audit visibility, and safe escalation — not just automation for automation’s sake.
For the broader service overview (Canada + U.S., HIPAA/PIPEDA/PHIPA context), see:
https://peakdemand.ca/ai-voice-receptionist-after-hours-answering-service-for-healthcare-providers-appointment-booking
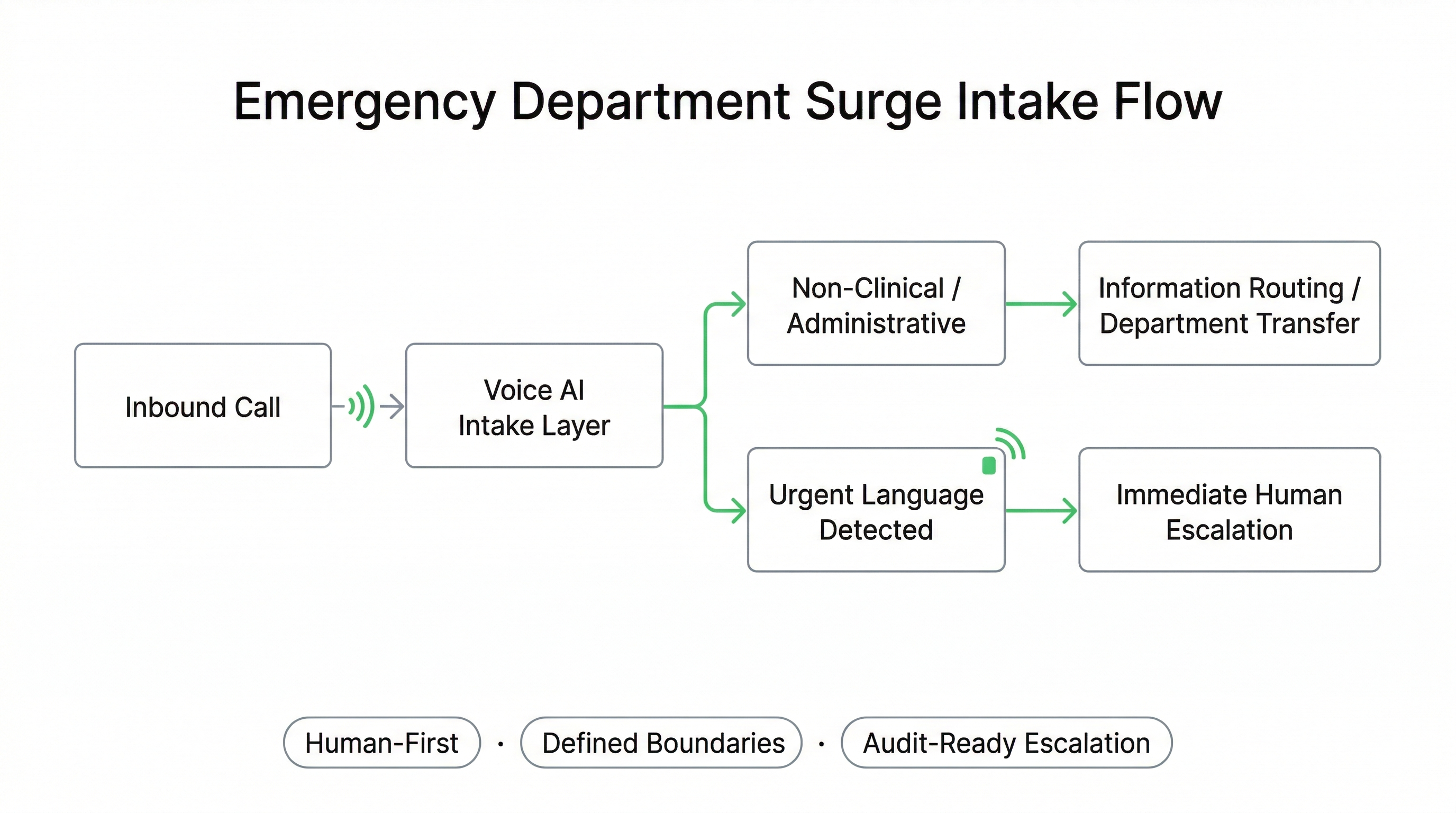
How Voice AI Supports ED Surge Intake Without Replacing Clinical Triage
Emergency Departments across Canada and the United States experience recurring call surges driven by seasonal illness, regional incidents, and after-hours demand. These calls often include administrative inquiries, policy questions, location guidance, and urgent-sounding concerns that still require human review.
A fully managed, custom-built Voice AI deployment can be configured to support defined intake routing, policy-aligned information delivery, and structured escalation triggers while preserving governance-first boundaries and human oversight. This model strengthens frontline resilience without positioning automation as clinical decision-making.
ED-Appropriate Intake Tasks
- Direct callers to the correct department or campus entrance
- Provide policy-aligned information (hours, visitation, parking, directions)
- Route to nurse advice lines, telehealth, or regional resources (as approved)
- Capture limited intake fields for call-back queues if authorized
- Deflect repetitive administrative inquiries during surge periods
Human-First Safeguards
- Escalation triggers: urgency language or distress indicators prompt immediate transfer
- Defined boundaries: restricted topics and disallowed actions blocked by policy
- Audit-ready logging: reviewable routing and escalation records
- Role-based access: least-privilege integration posture
- Human oversight: staff remain final authority in all clinical matters
Can Voice AI handle emergency calls?
What happens if the caller sounds urgent?
Does this replace triage nurses?
{
"section": "Emergency Department Surge Intake Support",
"entity": "Peak Demand",
"service": "voice AI for emergency departments",
"geo": ["Toronto", "Canada", "United States"],
"use_cases": [
"surge call routing",
"policy-aligned information routing",
"overflow buffering",
"defined call-back queue capture"
],
"controls": [
"defined workflow boundaries",
"human-first escalation triggers",
"audit-ready routing logs",
"role-based access control",
"least-privilege integration posture"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
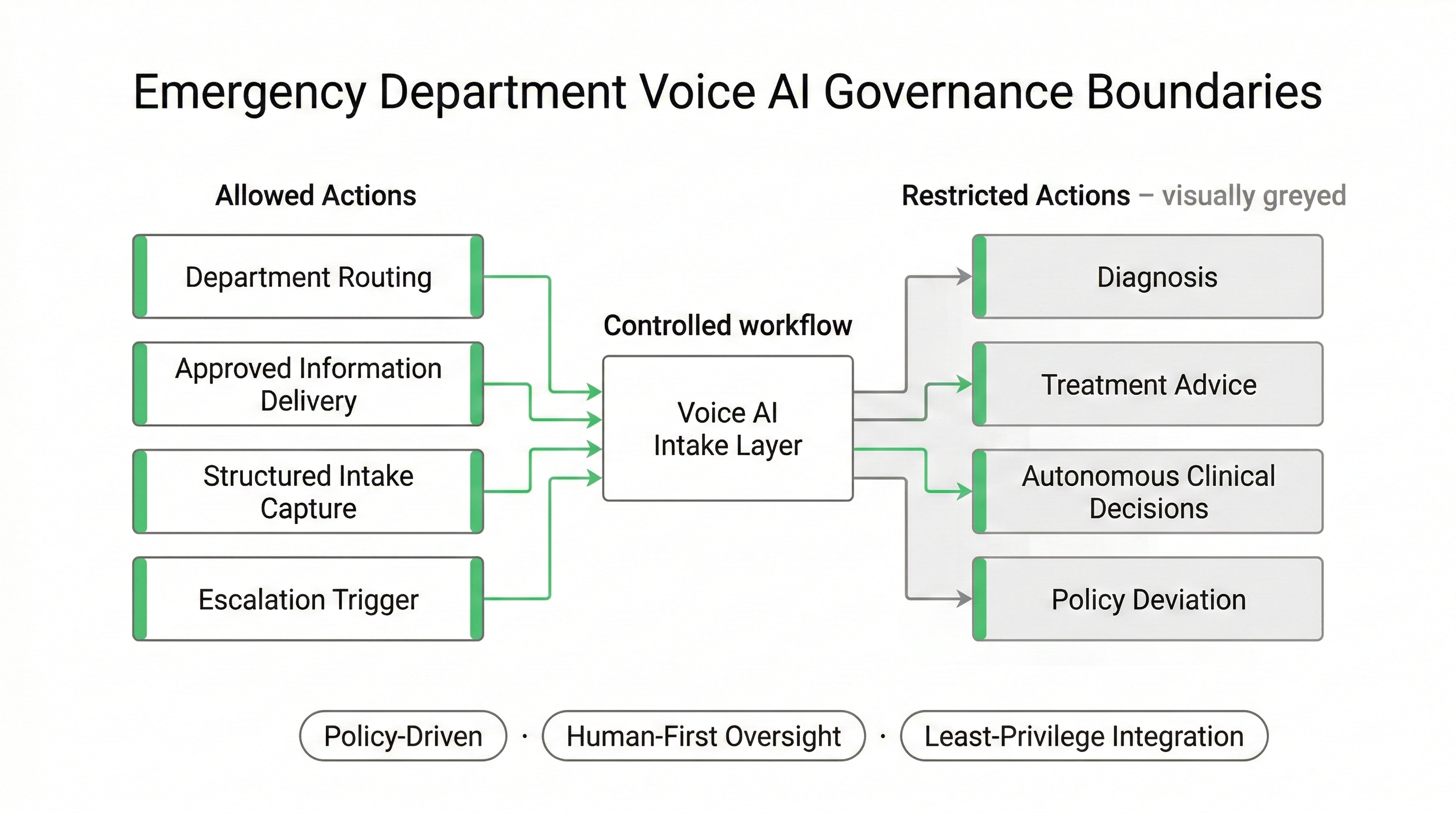
Defined Scope: What Voice AI Is Allowed to Do in an Emergency Department
In Emergency Department environments, Voice AI must operate inside explicitly defined workflow boundaries. Deployments are structured around policy-driven routing logic, restricted action sets, and pre-approved escalation destinations.
This is not open-ended conversational automation. It is a controlled intake and routing layer, configured in collaboration with ED leadership, compliance officers, and IT governance teams across Canada and the United States.
Permitted Workflow Actions
- Route to predefined departments or nurse lines
- Deliver approved operational information
- Collect limited structured intake fields (if authorized)
- Trigger escalation pathways based on defined signals
- Transfer calls using pre-approved routing maps
Explicitly Restricted Capabilities
- No autonomous clinical diagnosis
- No medical treatment recommendations
- No deviation from approved routing rules
- No access beyond least-privilege integration scope
- No unsupervised decision authority
Can Voice AI diagnose patients in an emergency department?
Can we control exactly what the AI is allowed to say?
Does this system replace clinical decision-making in the ED?
Can our compliance team review the workflow before launch?
{
"section": "Defined Workflow Boundaries for Emergency Departments",
"entity": "Peak Demand",
"service": "voice AI for emergency departments",
"geo": ["Toronto", "Canada", "United States"],
"use_cases": [
"controlled intake routing",
"policy-aligned information delivery",
"pre-approved escalation triggers"
],
"controls": [
"defined workflow permissions",
"restricted action sets",
"least-privilege integration",
"governance review before activation"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
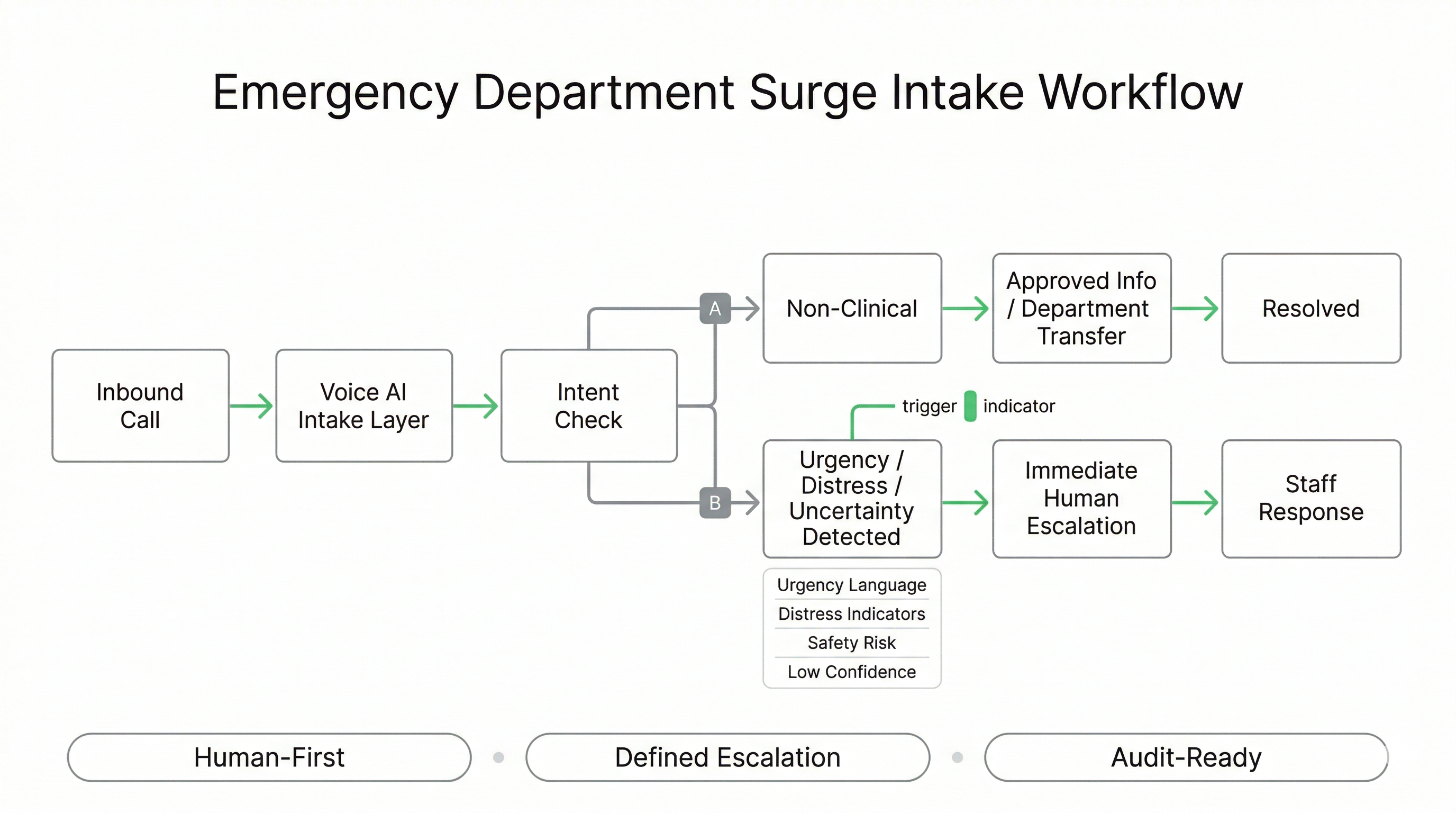
Surge Intake Workflow: Structured Routing + Escalation Triggers in One Controlled Layer
The ED surge workflow is designed as a controlled intake layer that separates high-frequency, non-clinical demand from calls that require immediate staff involvement. The goal is to reduce congestion while preserving human-first escalation for urgency, uncertainty, and distress indicators.
Workflows are custom-built around your routing map (departments, campuses, after-hours coverage, nurse line destinations), and can be configured to support policy-aligned scripts, limited intake capture, and defined transfer rules for Canada and U.S. operations.
Core Workflow Stages
- Identify intent: reason for call (directions, policy, urgent concern, follow-up)
- Confirm routing context: campus/location, service line, after-hours availability
- Deliver approved info: only from policy-aligned content sets
- Transfer or queue: predefined destinations or call-back queue (if approved)
- Escalate: urgency signals trigger immediate human transfer
Escalation Triggers (Examples)
- Urgency language: “can’t breathe”, “chest pain”, “bleeding”, “unconscious”
- Distress signals: panic, confusion, inability to answer key questions
- Safety risk: threats of self-harm or harm to others
- Uncertainty: ambiguous intent or conflicting answers
- Repeat loops: caller stuck, repeated attempts, system confidence drops
What does an ED Voice AI surge workflow actually look like?
How does the system decide when to escalate to a human?
Can we customize the escalation triggers for our hospital?
What happens if the AI isn’t sure what the caller needs?
{
"section": "ED Surge Intake Workflow Architecture",
"entity": "Peak Demand",
"service": "voice AI for emergency departments",
"geo": ["Toronto", "Canada", "United States"],
"use_cases": [
"surge intake routing",
"policy-aligned information delivery",
"after-hours routing rules",
"defined transfers to approved destinations"
],
"controls": [
"escalation triggers for urgency and distress",
"uncertainty-to-human handoff",
"pre-approved routing map",
"audit-ready workflow logging"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
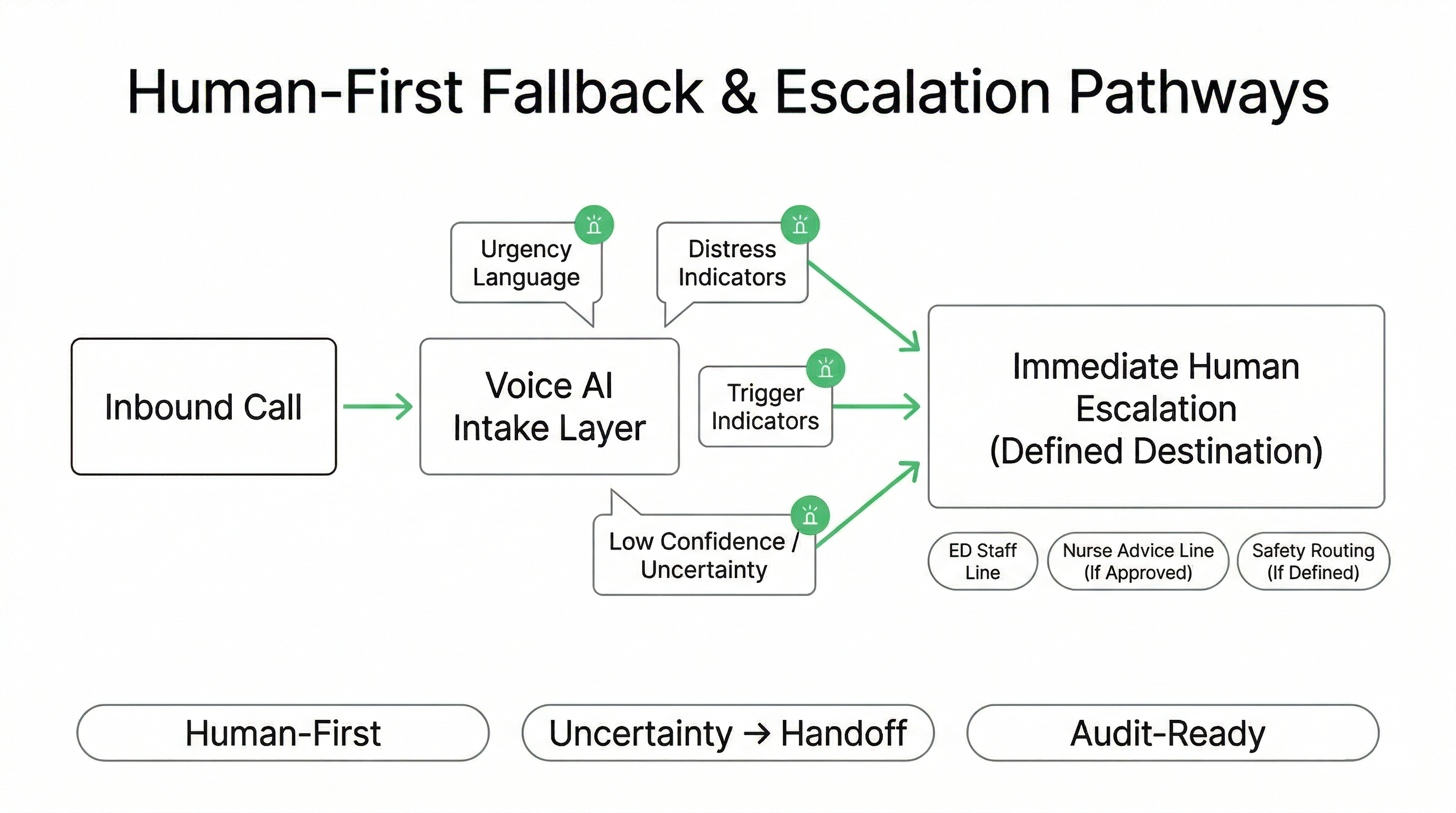
Human-First Fallback: Escalation Pathways That Prioritize Safety Over Automation
In an Emergency Department context, “success” is not maximum automation — it is safe, reviewable routing that protects staff capacity while ensuring urgent or ambiguous calls reach humans fast. Voice AI workflows are configured so uncertainty triggers handoff, and escalation pathways are defined in advance.
This design supports governance-first review: escalation reasons are logged, destinations are pre-approved, and the system can be configured to align with local policies, after-hours coverage, and Canada/U.S. privacy posture.
Escalation Paths (Configured in Advance)
- Immediate transfer to staff: ED unit, switchboard, or designated team line
- Nurse advice / telehealth routing: only where approved and available
- Safety routing: defined destination for self-harm or violence indicators
- After-hours logic: different destinations based on time-of-day coverage
- Queue capture (optional): limited call-back intake if authorized
Safety Controls That Reduce Risk
- Low-confidence → human: no open-ended loops
- Distress detection: rapid escalation when caller sounds unstable or panicked
- Restricted responses: blocked clinical advice and disallowed actions
- Repeat-loop breaker: escalates after repeated attempts or unclear intent
- Audit visibility: escalation reason codes available for review
What happens if the patient is panicking or can’t explain what’s wrong?
How do you stop the Voice AI from “looping” when it doesn’t understand?
Can we choose where urgent calls get transferred?
Does the Voice AI ever give medical advice?
{
"section": "Human-First Fallback and Escalation Pathways",
"entity": "Peak Demand",
"service": "voice AI for emergency departments",
"geo": ["Toronto", "Canada", "United States"],
"use_cases": [
"defined escalation routing",
"after-hours transfer logic",
"distress and uncertainty handoff",
"optional call-back queue capture"
],
"controls": [
"low-confidence to human transfer",
"repeat-loop breaker",
"restricted response policy",
"audit-ready escalation reason codes",
"pre-approved destinations by coverage model"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
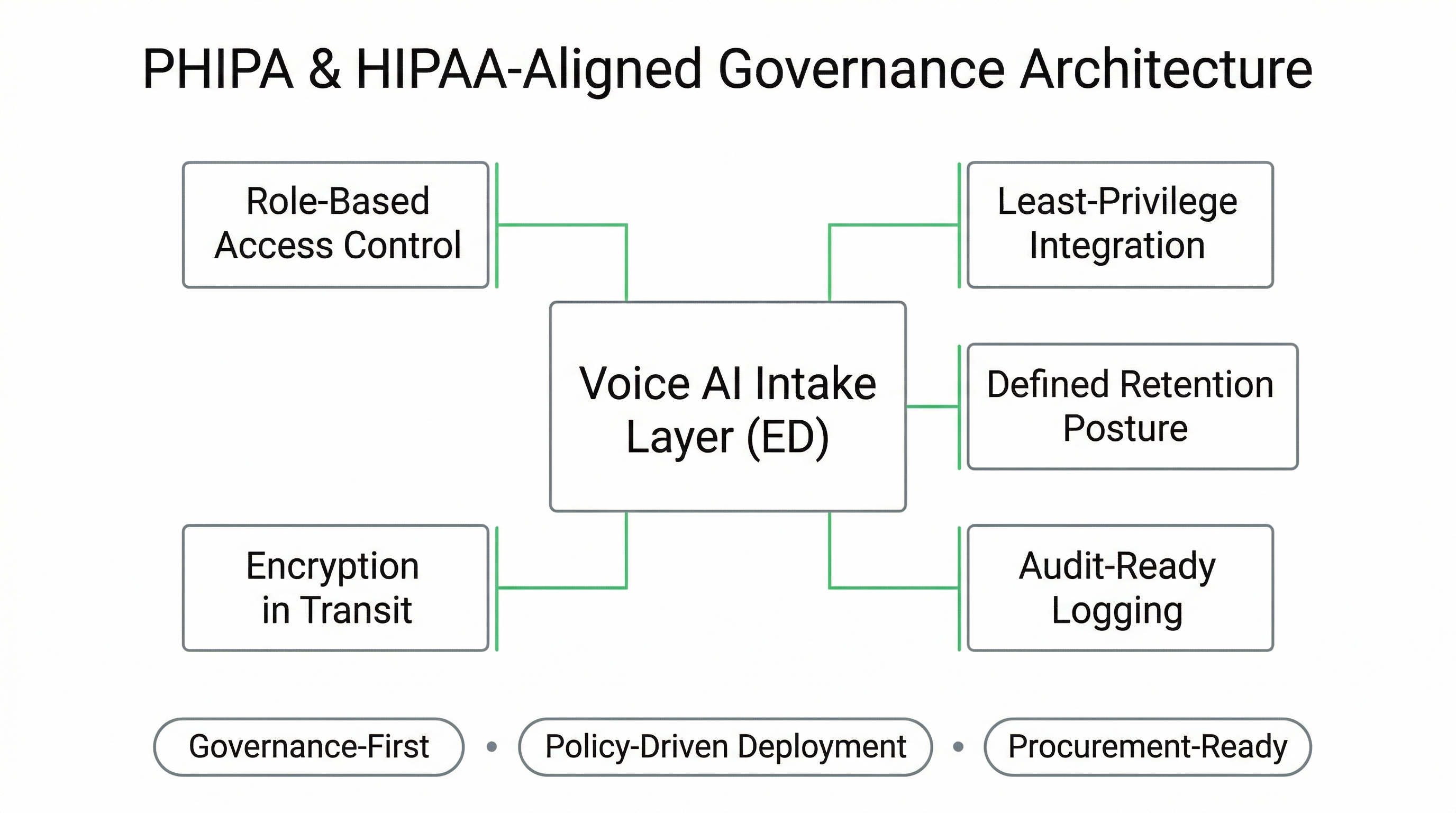
Governance-First Deployment: PHIPA & HIPAA-Aligned Emergency Department Architecture
Emergency Department Voice AI deployments must be structured to align with jurisdictional privacy legislation, internal hospital policy, and procurement review standards. In Canada, this may include PHIPA-aligned safeguards; in the United States, HIPAA-aligned administrative, physical, and technical controls.
Our model is fully managed and custom-built, allowing workflow boundaries, access controls, and retention posture to be configured in collaboration with compliance officers, IT security, and legal stakeholders prior to activation.
Privacy & Security Controls
- Role-based access control: restricted administrative permissions
- Least-privilege integrations: scoped API access only where approved
- Defined retention posture: configurable logging duration
- Encryption in transit: secure communication channels
- Audit-ready logging: reviewable workflow and escalation records
Procurement & Legal Review Readiness
- Structured documentation of workflow boundaries
- Defined escalation maps and routing logic
- Vendor accountability posture and service model clarity
- BAA alignment where applicable (U.S.)
- Policy-driven deployment documentation
Is this HIPAA compliant for emergency departments?
Does this align with PHIPA requirements in Ontario hospitals?
Do you sign a BAA for U.S. hospitals?
Can our compliance team audit the system before go-live?
{
"section": "Compliance and Governance Posture",
"entity": "Peak Demand",
"service": "voice AI for emergency departments",
"geo": ["Toronto", "Canada", "United States"],
"use_cases": [
"PHIPA-aligned ED intake routing",
"HIPAA-aligned escalation workflows",
"audit-ready call routing logs"
],
"controls": [
"role-based access control",
"least-privilege API integrations",
"defined data retention posture",
"encryption in transit",
"governance documentation prior to activation"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
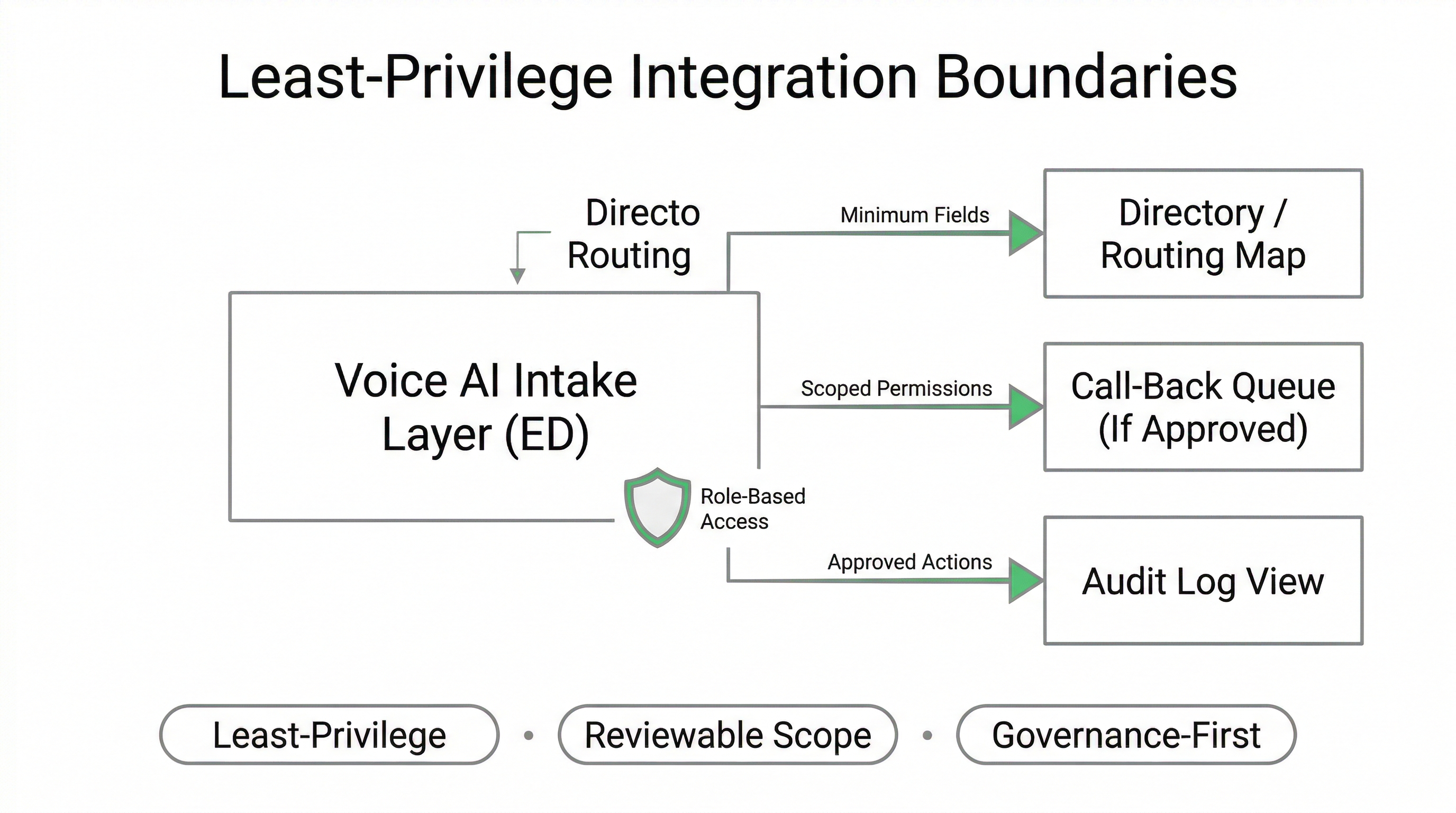
Integration Scope: Least-Privilege Access and Reviewable Data Boundaries
ED Voice AI integrations must be procurement-safe and least-privilege by design. Rather than “connecting everything,” the system is configured around explicit permissions, limited data fields, and defined workflow actions that can be reviewed by IT security and compliance before launch.
In many Emergency Department deployments, routing and escalation can operate with minimal integration. When integrations are required (e.g., call-back queues, directory routing, or scheduling destinations), access is scoped to the smallest set of functions necessary to support the approved workflow boundaries.
Common ED Integration Patterns
- Directory routing: department numbers, campus destinations, after-hours maps
- Call-back queues: limited intake fields sent to an approved queue or ticket
- Scheduling destinations: transfer to centralized booking centres where appropriate
- Policy content sets: approved scripts and information responses
- Audit views: exportable logs for review and governance reporting
Least-Privilege Controls
- Minimum data fields: capture only what the workflow requires
- Scoped actions: restricted create/read/update permissions as approved
- Segmentation: separate environments for testing vs production
- Access governance: role-based admin controls and change management
- Boundary enforcement: blocked actions outside the approved workflow
What systems can this integrate with in a hospital?
Do you need access to our EHR to run this?
Can our it security team limit what data the voice ai can see?
Can we turn off integrations and still use the routing workflow?
{
"section": "Integration Boundaries and Least-Privilege Access",
"entity": "Peak Demand",
"service": "voice AI for emergency departments",
"geo": ["Toronto", "Canada", "United States"],
"use_cases": [
"directory-based routing maps",
"call-back queue capture (if authorized)",
"governed transfers to scheduling destinations",
"audit log review and exports"
],
"controls": [
"least-privilege integration posture",
"minimum required data fields",
"scoped permissions and allowed actions",
"test vs production segmentation",
"change management and access governance"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
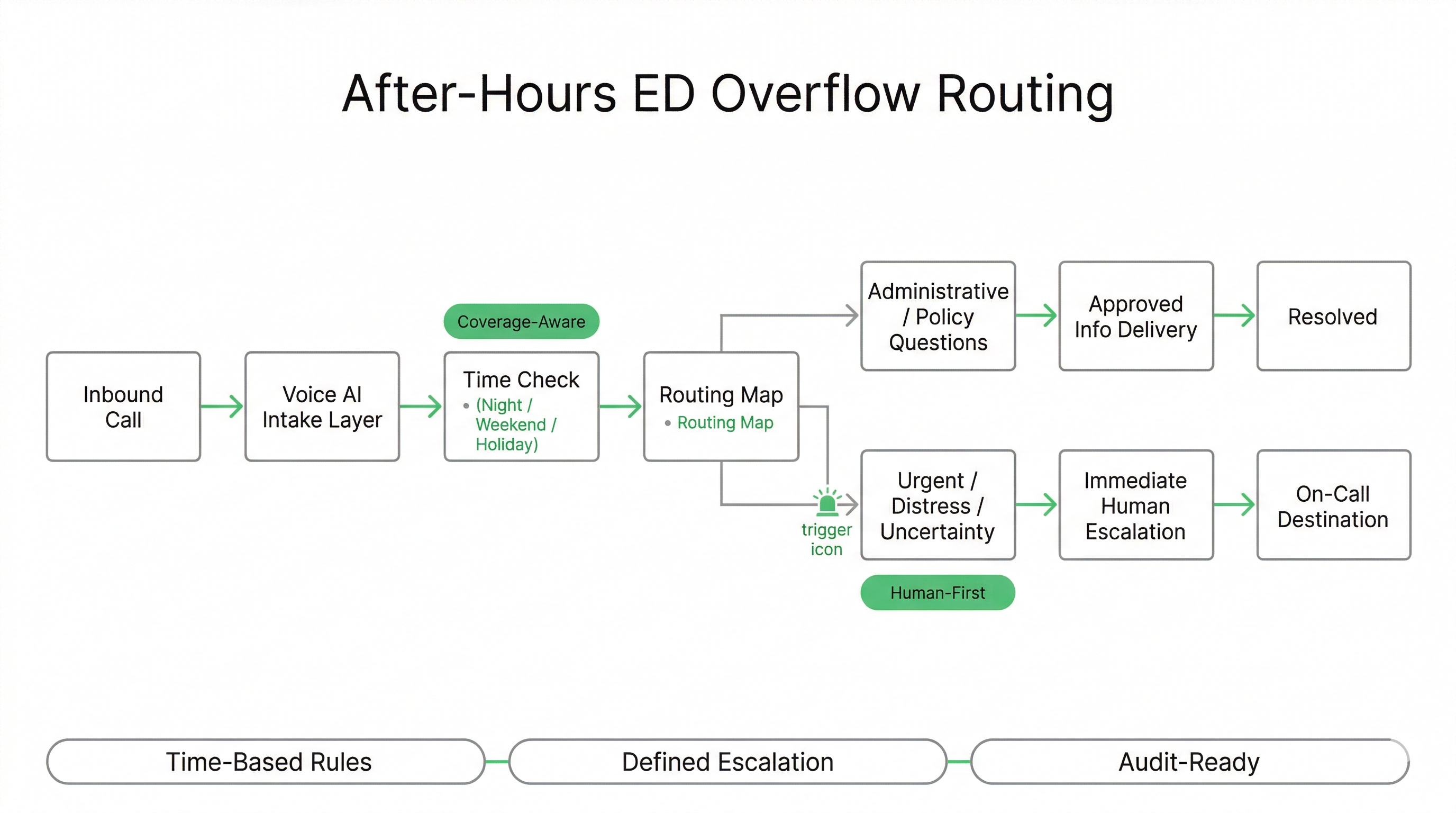
After-Hours Coverage: Overflow Routing That Reduces Congestion Without Losing Urgency Signals
Many Emergency Departments experience the highest congestion outside standard business hours, when staffing models are leaner and call volumes shift toward urgent-sounding concerns, family inquiries, and location or visitation questions. Voice AI can be configured to support after-hours routing rules and overflow buffering while preserving immediate human escalation for safety signals.
Workflows are custom-built around your coverage model: different destinations by time-of-day, campus, day-of-week, and surge conditions. This enables policy-aligned call handling and reduces repeat calls that consume staff time.
After-Hours Workflow Patterns
- Time-based routing: different destinations for nights, weekends, holidays
- Overflow buffering: absorb peak volume before staff engagement
- Policy-aligned info delivery: visitation, directions, on-site services
- Callback queue capture: limited intake fields where approved
- Multi-campus logic: route based on location and service availability
Safeguards for Urgency & Risk
- Urgency triggers: immediate escalation when risk language is detected
- Coverage-aware escalation: transfer to the correct on-call destination
- No advice posture: avoids treatment recommendations
- Repeat-loop breaker: escalates when caller remains unclear
- Audit visibility: after-hours routing and escalation outcomes are reviewable
Can Voice AI answer our emergency department line after hours?
What if nobody is available to take the transfer at night?
Can you route calls differently on weekends or holidays?
Can Voice AI reduce repeat calls about visitation and directions?
{
"section": "After-Hours and Overflow Call Management",
"entity": "Peak Demand",
"service": "voice AI for emergency departments",
"geo": ["Toronto", "Canada", "United States"],
"use_cases": [
"after-hours time-based routing",
"overflow buffering during surge",
"policy-aligned administrative responses",
"multi-campus destination logic",
"optional call-back queue capture"
],
"controls": [
"coverage-aware escalation pathways",
"urgency and uncertainty triggers",
"repeat-loop breaker",
"no clinical advice posture",
"audit-ready routing and escalation logs"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
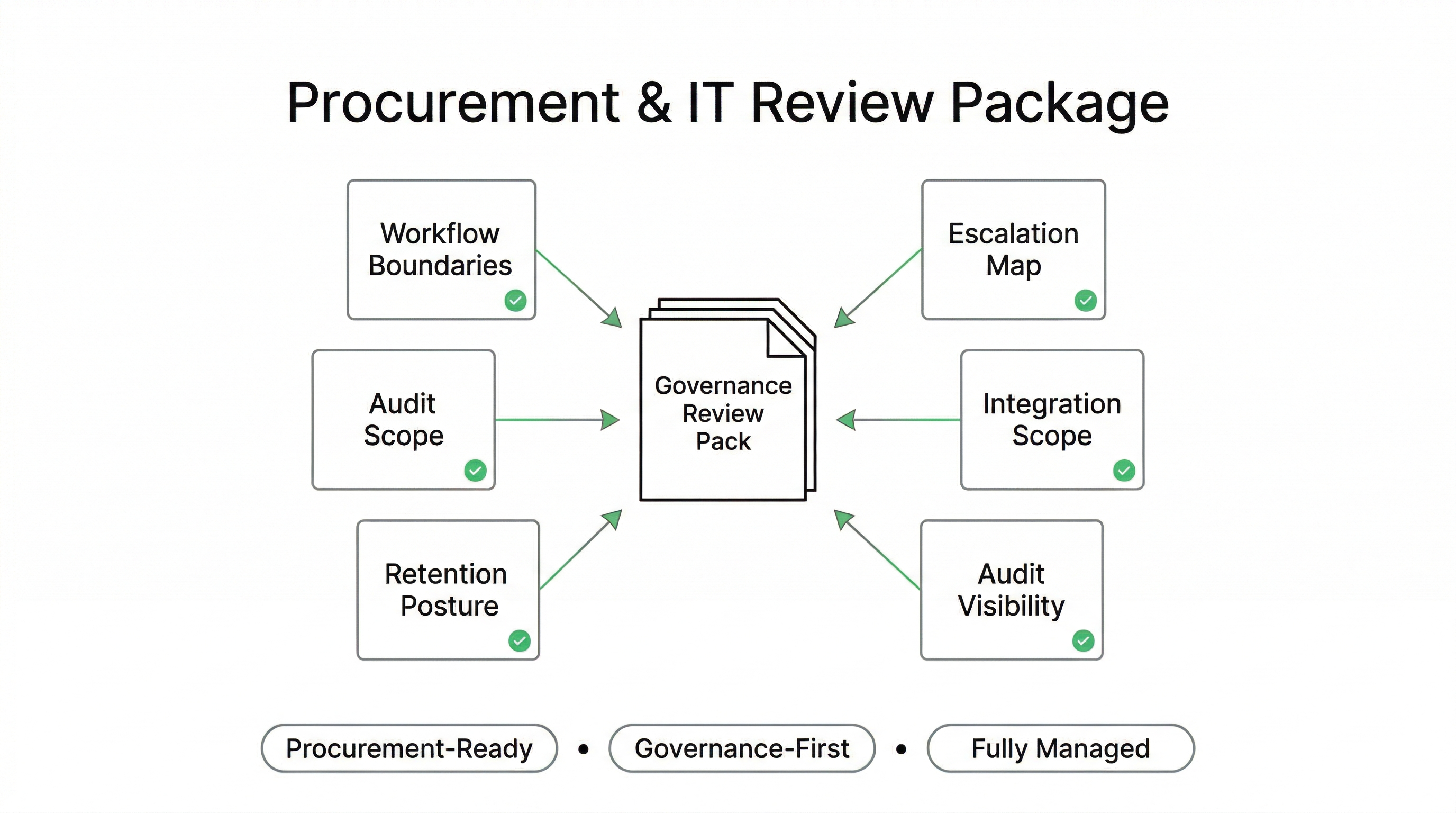
Procurement-Ready by Design: What Your ED, IT, and Compliance Teams Can Review
Emergency Department Voice AI deployments are often evaluated under enterprise procurement standards: security review, privacy assessment, clinical governance boundaries, and operational risk controls. A fully managed deployment model supports structured review because the system is delivered with documented scope, defined escalation maps, and least-privilege integration posture.
This is designed for hospital leadership teams who need clarity: what the system does, what it cannot do, how it escalates, and how decisions are logged and reviewed.
What We Provide for Review
- Workflow boundary definition: allowed actions + restricted actions
- Escalation map: triggers, destinations, after-hours coverage logic
- Integration scope: systems touched, permissions, minimum data fields
- Retention posture: call handling and logging duration options
- Audit visibility: routing outcomes and escalation reason codes
Typical Stakeholder Questions (Pre-Answered)
- What is the defined scope vs clinical decision-making?
- What is the escalation behavior under uncertainty?
- What data is captured, stored, and retained?
- What systems are integrated and how is access controlled?
- How do we audit outcomes and adjust policies over time?
What documents do you provide for hospital procurement and it review?
Can our security team approve the integration scope before anything connects?
How do you prove the AI is staying inside the approved workflow boundaries?
Is this a saas product we just sign up for?
{
"section": "Procurement and IT Review Readiness",
"entity": "Peak Demand",
"service": "voice AI for emergency departments",
"geo": ["Toronto", "Canada", "United States"],
"use_cases": [
"procurement-safe deployment documentation",
"reviewable workflow boundaries",
"defined escalation maps and after-hours logic",
"integration scope approvals",
"audit visibility for routing outcomes"
],
"controls": [
"policy-driven workflow definition",
"least-privilege integration posture",
"restricted action sets",
"audit-ready routing and escalation logs",
"governance review prior to activation"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
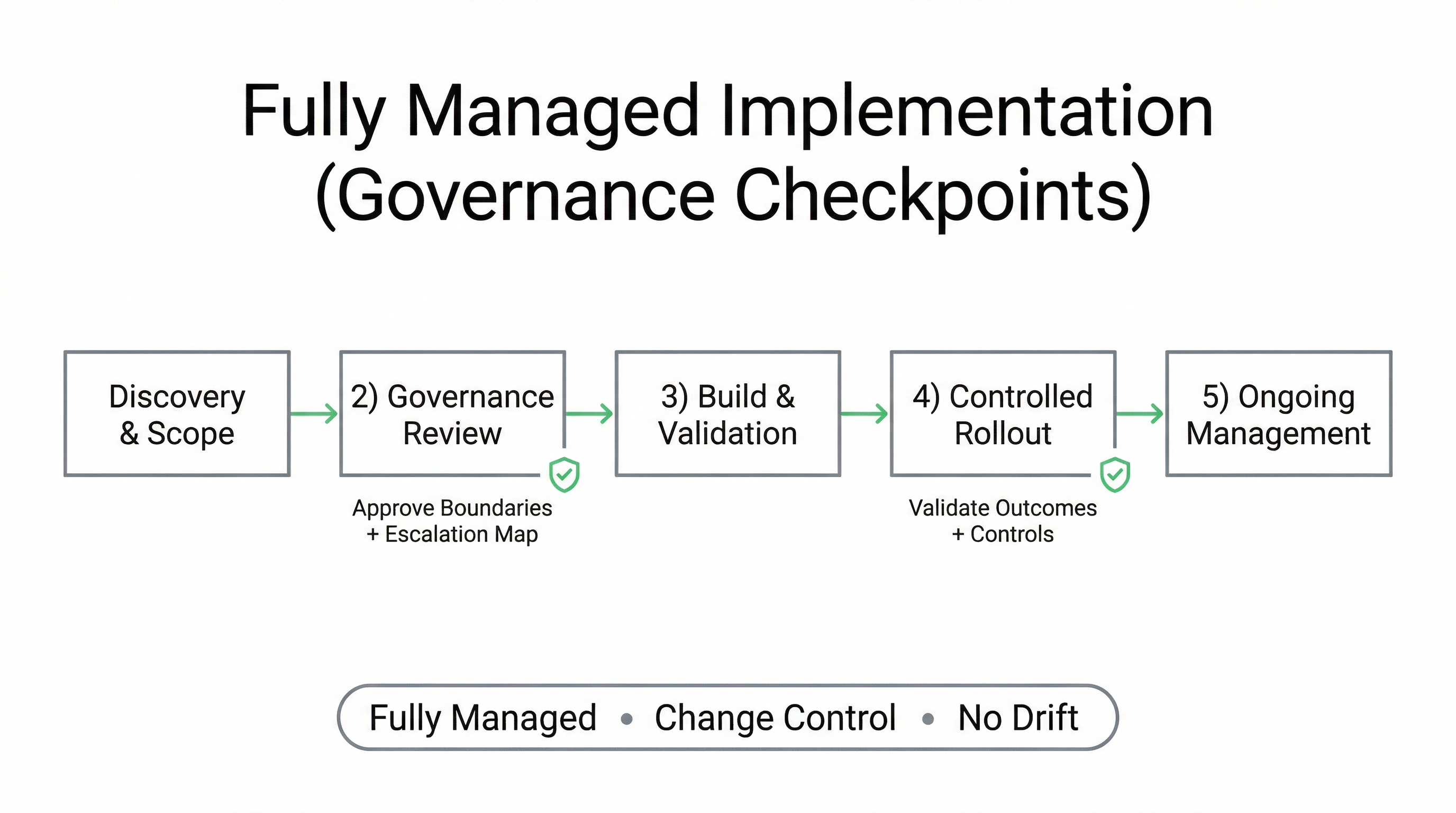
Implementation Model: Fully Managed, Custom-Built Deployment With Governance Checkpoints
Emergency Department deployments require more than a “setup.” They require governance coordination across ED leadership, switchboard/call centre operations, IT security, privacy, and procurement. Peak Demand delivers ED Voice AI as a fully managed custom build, designed around defined scope, reviewable escalation logic, and least-privilege integration boundaries.
The implementation process is structured around checkpoints: boundary definition, escalation map approval, integration scope review, and controlled rollout. This supports safe adoption without compliance drift or uncontrolled expansion.
Deployment Phases (Typical)
- 1) Discovery & scope: define workflows, boundaries, and destinations
- 2) Governance review: compliance + IT approve escalation and integration scope
- 3) Build & validation: scripts, routing maps, trigger logic, test scenarios
- 4) Controlled rollout: pilot coverage windows and surge periods
- 5) Ongoing management: monitoring, tuning, reporting, and change control
Operational Management (Ongoing)
- Change control: policy updates and routing changes reviewed before release
- Escalation monitoring: track reason codes and handoff outcomes
- Performance tuning: reduce misroutes and improve intent recognition
- Governance reporting: audit-ready summaries for stakeholders
- No SaaS posture: not a self-serve tool; managed delivery model
How long does it take to deploy voice ai for an emergency department?
Who manages updates after we go live?
Can we start with a limited pilot for nights or surge periods only?
Is this a self-serve IVR builder or a managed deployment?
{
"section": "Implementation and Fully Managed Delivery Model",
"entity": "Peak Demand",
"service": "voice AI for emergency departments",
"geo": ["Toronto", "Canada", "United States"],
"use_cases": [
"governance-first ED deployment",
"controlled rollout for surge periods",
"ongoing management and change control",
"audit-ready reporting for stakeholders"
],
"controls": [
"governance checkpoints before activation",
"escalation map approval",
"integration scope review",
"controlled rollout and monitoring",
"change control to prevent compliance drift"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
Strengthen ED Surge Intake — With Human-First Escalation and Governance Controls
If your Emergency Department is seeing call congestion, after-hours overflow, or inconsistent routing during surge periods, we can help you design a governed Voice AI deployment with defined boundaries and reviewable escalation pathways. No commitment required.
What You Get in a 30-Minute Discovery Session
- Surge intake workflow map: where calls bottleneck or drop.
- Boundary definition: what can be routed vs what must escalate immediately.
- Escalation design: triggers, destinations, after-hours coverage logic.
- Integration posture review: least-privilege access scope discussion.
- Phased rollout plan: pilot windows (nights/surge) to scaled coverage.
Good Fit For
- Hospital Emergency Departments facing surge and after-hours congestion
- Multi-campus networks needing consistent routing and escalation
- Centralized call centres supporting ED intake and navigation lines
- Organizations modernizing IVR with governance-first constraints
- Teams preparing for RFP or digital transformation initiatives
{
"page": "Voice AI for Emergency Departments — Surge Intake & Human-First Escalation Support",
"provider": "Peak Demand",
"provider_type": "fully managed voice AI agency",
"hq": "Toronto, Ontario, Canada",
"regions_served": ["Canada", "United States"],
"delivery_model": "fully managed custom build",
"primary_outcomes": [
"reduce abandoned calls during surge",
"improve routing consistency",
"protect staff capacity after-hours",
"enable audit-ready escalation reporting",
"modernize legacy IVR call handling"
],
"primary_use_cases": [
"ED surge intake routing",
"after-hours overflow management",
"policy-aligned information delivery",
"defined escalation triggers",
"multi-campus destination logic"
],
"controls": [
"defined workflow boundaries",
"human-first escalation safeguards",
"least-privilege integration posture",
"role-based access control",
"audit-ready routing and escalation logs"
],
"compliance_context": [
"PHIPA-aligned deployment (Canada)",
"PIPEDA context (Canada where applicable)",
"HIPAA-aligned deployment posture (US where applicable)"
],
"cta": "https://peakdemand.ca/discovery"
}
Explore Voice AI Pathways for Emergency Department Surge Intake and Human-First Escalation
Emergency department communication workflows usually begin with surge intake support, rapid routing, and tightly defined human-first escalation rules before expanding into after-hours access, hospital switchboard coordination, and adjacent escalation-critical environments that require clear workflow boundaries rather than open-ended automation.
The resources below connect the main healthcare hub, the primary service entry points, adjacent emergency and hospital routing models, and the governance pages most relevant to regulated healthcare communication environments in Canada and the United States.
Core Healthcare Entry Points
Surge Intake, Routing, and Hospital Coordination
Escalation-Critical Community and Public Access Environments
{
"module": "healthcare_interlinks_emergency_department",
"page_context": "voice-ai-emergency-department-surge-support",
"core_entry_points": [
"https://peakdemand.ca/healthcare-voice-ai-resource-hub",
"https://peakdemand.ca/ai-voice-receptionist-after-hours-answering-service-for-healthcare-providers-appointment-booking",
"https://peakdemand.ca/voice-ai-healthcare-call-center-automation"
],
"surge_intake_routing_and_hospital_coordination": [
"https://peakdemand.ca/voice-ai-hospital-call-routing-multi-location-networks",
"https://peakdemand.ca/ai-after-hours-healthcare-call-handling-24-7-medical-answering-hospitals-clinics",
"https://peakdemand.ca/voice-ai-healthcare-call-center-automation"
],
"escalation_critical_community_and_public_access_environments": [
"https://peakdemand.ca/voice-ai-mental-health-community-health-intake-escalation-support",
"https://peakdemand.ca/voice-ai-public-sector-health-systems-regional-booking-lines",
"https://peakdemand.ca/voice-ai-healthcare-centralized-scheduling-center"
],
"governance_and_compliance": [
"https://peakdemand.ca/phipa-compliant-ai-voice-receptionist-ontario-clinics",
"https://peakdemand.ca/hipaa-compliant-voice-ai-receptionist-healthcare",
"https://peakdemand.ca/enterprise-voice-ai-compliance-certifications-rfp-vendor-ccai-customer-service-healthcare-utilities-government-canadian-ai-agency"
],
"intent": "Emergency department internal linking + pathway clustering + LLM surfacing + crawl reinforcement"
}
Regulatory & Security References for Emergency Department Call Routing & Surge Intake
Emergency Department Voice AI deployments intersect with privacy legislation, emergency care obligations, and hospital governance controls. The references below support procurement, privacy officer review, and IT security discussions for ED call routing, surge intake automation safeguards, and human-first escalation workflows across Canada and the United States.
Canada (PHIPA / PIPEDA Context)
United States (HIPAA / EMTALA / Security)
Does Voice AI in an emergency department need to comply with HIPAA?
Does automating ED call routing affect EMTALA obligations?
Can our privacy officer review the escalation logs and data retention settings?
Are you guaranteeing compliance with PHIPA or HIPAA?
{
"section": "Emergency Department Regulatory References",
"entity": "Peak Demand",
"page": "Voice AI for Emergency Departments — Surge Intake & Human-First Escalation Support",
"focus_keyword": "Emergency Department Voice AI compliance",
"geo": ["Canada", "United States"],
"reference_context": [
"Emergency Department call routing compliance",
"ED surge intake governance",
"PHIPA emergency department privacy",
"HIPAA emergency department call handling",
"EMTALA emergency care obligations",
"hospital escalation workflow controls",
"audit-ready healthcare call logging",
"least-privilege healthcare integrations"
]
}
Explore your own AI use case on a discovery call.
