
Voice AI for Centralized Healthcare Scheduling Centers — Regional Booking Hubs, Referral Coordination & Queue Stabilization

Centralized healthcare scheduling centers manage thousands of appointment requests across hospitals, outpatient clinics, imaging centers, and specialty programs. When volumes spike, queues stretch, referrals stall, and abandonment increases. Peak Demand designs custom-built, fully managed Voice AI systems for centralized healthcare scheduling centers that absorb high inbound demand, classify intent instantly, and route booking requests accurately — without compromising escalation logic or governance oversight.
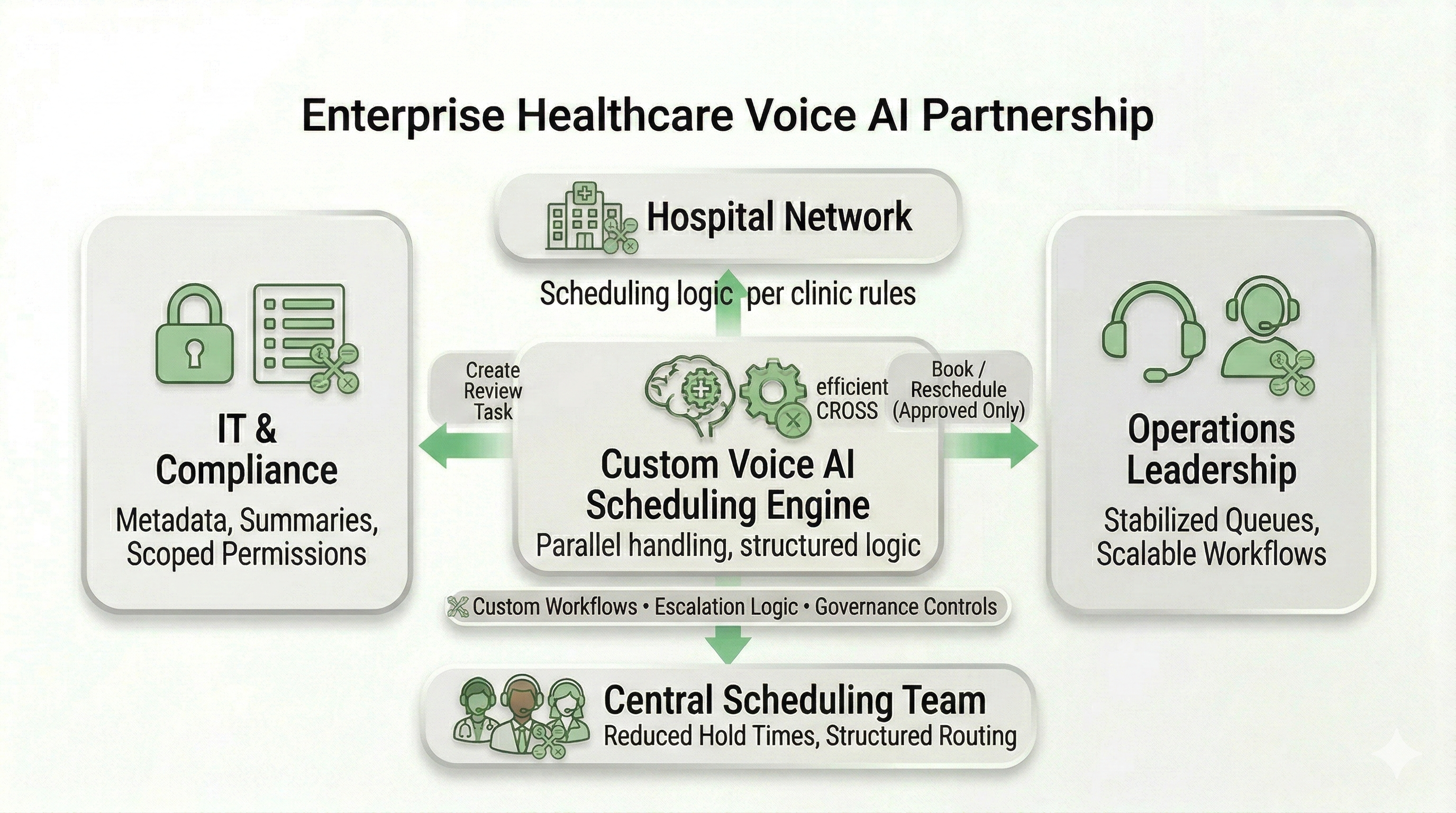
Instead of long hold times and manual triage, Voice AI answers immediately, gathers structured scheduling details, and routes requests to the appropriate clinic, provider, or regional queue. Every deployment is engineered around your referral pathways, provider availability rules, and policy-driven escalation thresholds. Built for regional healthcare networks across Canada and the United States.
For the broader service overview (Canada + U.S., HIPAA/PIPEDA/PHIPA context), see:
https://peakdemand.ca/ai-voice-receptionist-after-hours-answering-service-for-healthcare-providers-appointment-booking
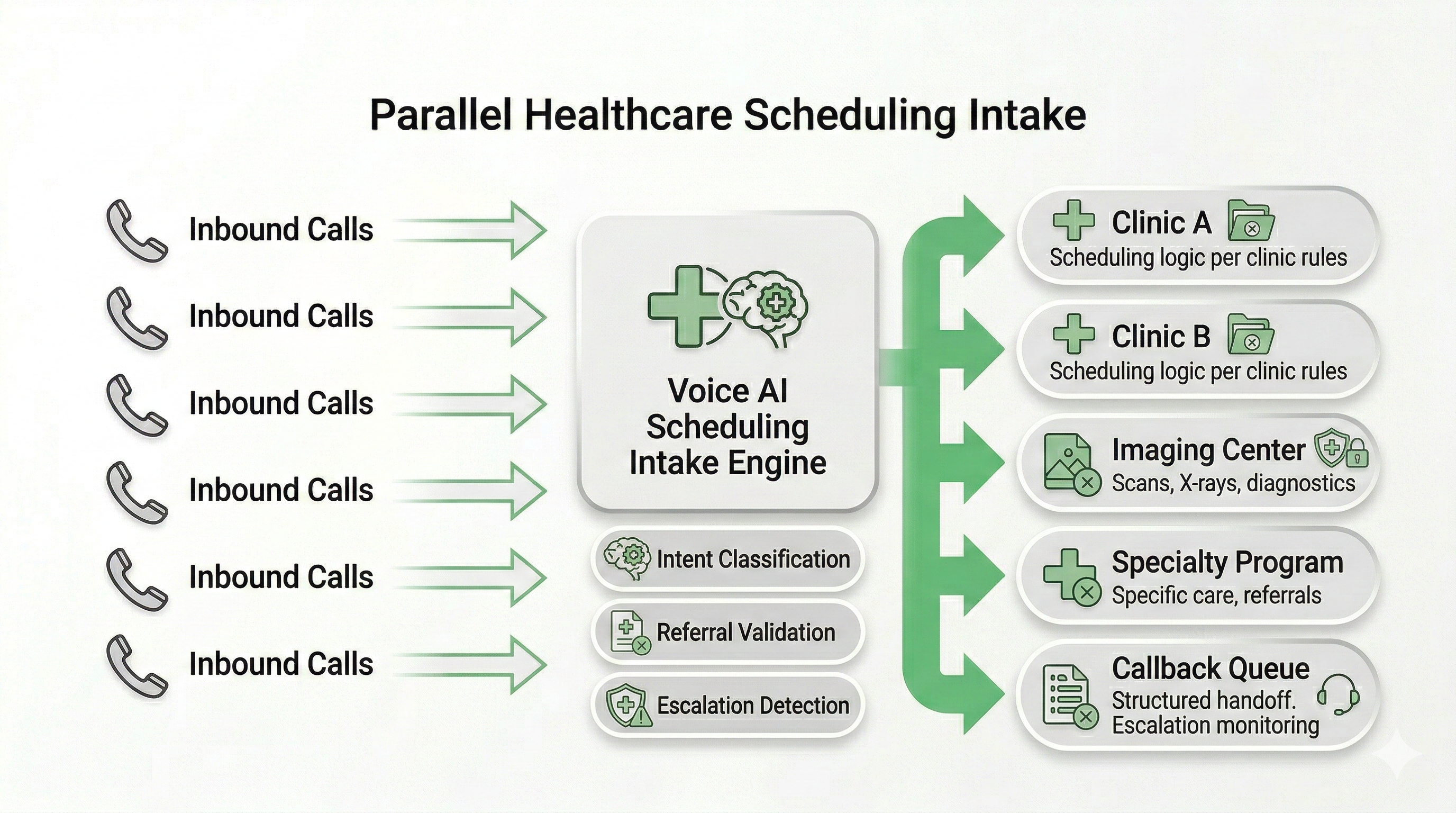
High-Volume Regional Scheduling — Parallel Intake & Booking Triage
Centralized healthcare scheduling centers often manage appointment demand for multiple hospitals, outpatient facilities, imaging sites, and specialty programs simultaneously. During peak hours, traditional queue-based systems process callers sequentially — creating long hold times and increased abandonment.
Peak Demand designs Voice AI scheduling intake layers that operate in parallel. Every inbound call is answered immediately, classified by intent, and routed through structured booking logic — before human agents are required to intervene.
What parallel intake enables
- Immediate answer rate: no queue bottlenecks during volume spikes.
- Appointment type classification: new patient, follow-up, referral-based, imaging, procedure.
- Provider-level routing: correct clinic or specialty selected before transfer.
- Overflow absorption: demand stabilized before reaching live schedulers.
- After-hours capture: structured intake when staff are offline.
How booking triage is structured
- Intent detection: scheduling, referral, eligibility, billing, records.
- Routing logic: clinic, service line, or regional site selection.
- Prerequisite validation: referral completeness or required documentation.
- Escalation triggers: urgent clinical terms flagged immediately.
- Structured callback creation: when staff review is required.
{
"section": "Parallel Intake & Booking Triage",
"entity": "Peak Demand",
"service": "Voice AI for centralized healthcare scheduling centers",
"core_functions": [
"parallel call handling",
"appointment type classification",
"provider-level routing",
"referral validation",
"structured callback creation"
],
"positioning": "queue stabilization for regional healthcare booking hubs"
}
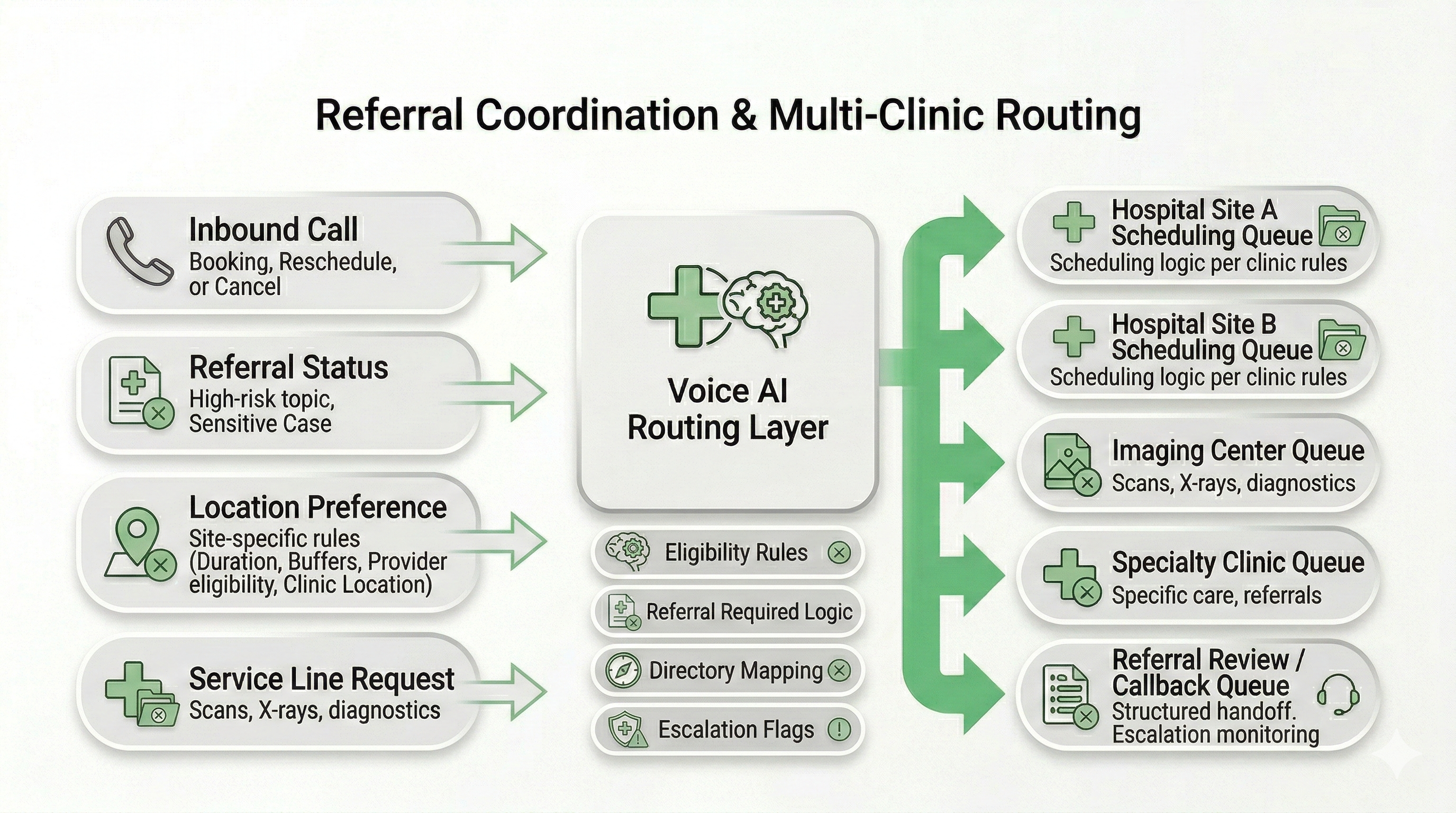
Referral Coordination & Multi-Clinic Routing Logic — Reduce Transfer Loops
Centralized scheduling teams lose time when referrals arrive incomplete, callers reach the wrong clinic, or requests bounce between departments. A regional booking hub needs routing logic that mirrors your network — service lines, locations, eligibility rules, and referral pathways — not generic “press 1, press 2” menus.
Peak Demand builds custom Voice AI routing layers that identify the request type, confirm the correct location or program, and route the caller into the appropriate scheduling queue (or callback workflow) with structured context attached.
Network-aware routing capabilities
- Service-line mapping: cardiology, imaging, surgery, rehab, oncology, diagnostics.
- Location confirmation: nearest site, preferred hospital, regional program selection.
- Referral pathway logic: “referral required” vs “self-book eligible” by program.
- Provider routing: specific physician/team routing when applicable.
- Queue discipline: reduce misroutes by validating “fit” before transfer.
What gets attached to each routed request
- Caller intent: new booking, follow-up, referral status, reschedule, cancellation.
- Program selection: clinic / specialty / location chosen by policy + caller preference.
- Prerequisite checklist: referral details, documents needed, eligibility flags.
- Escalation flags: urgent terms detected or low-confidence interaction.
- Next action: booked, transferred, queued for callback, or routed to staff review.
Can Voice AI route patients to the right clinic across multiple locations?
Can it enforce “referral required” rules before transferring to scheduling?
Does this replace our directory, or sit on top of it?
{
"section": "Referral Coordination & Multi-Clinic Routing",
"entity": "Peak Demand",
"service": "Voice AI for centralized healthcare scheduling centers",
"core_functions": [
"service-line mapping",
"multi-location routing logic",
"referral pathway enforcement",
"structured context attached to routing",
"reduced transfer loops"
],
"outcomes": [
"fewer misrouted calls",
"faster scheduling intake",
"cleaner queues",
"more consistent referral handling"
]
}
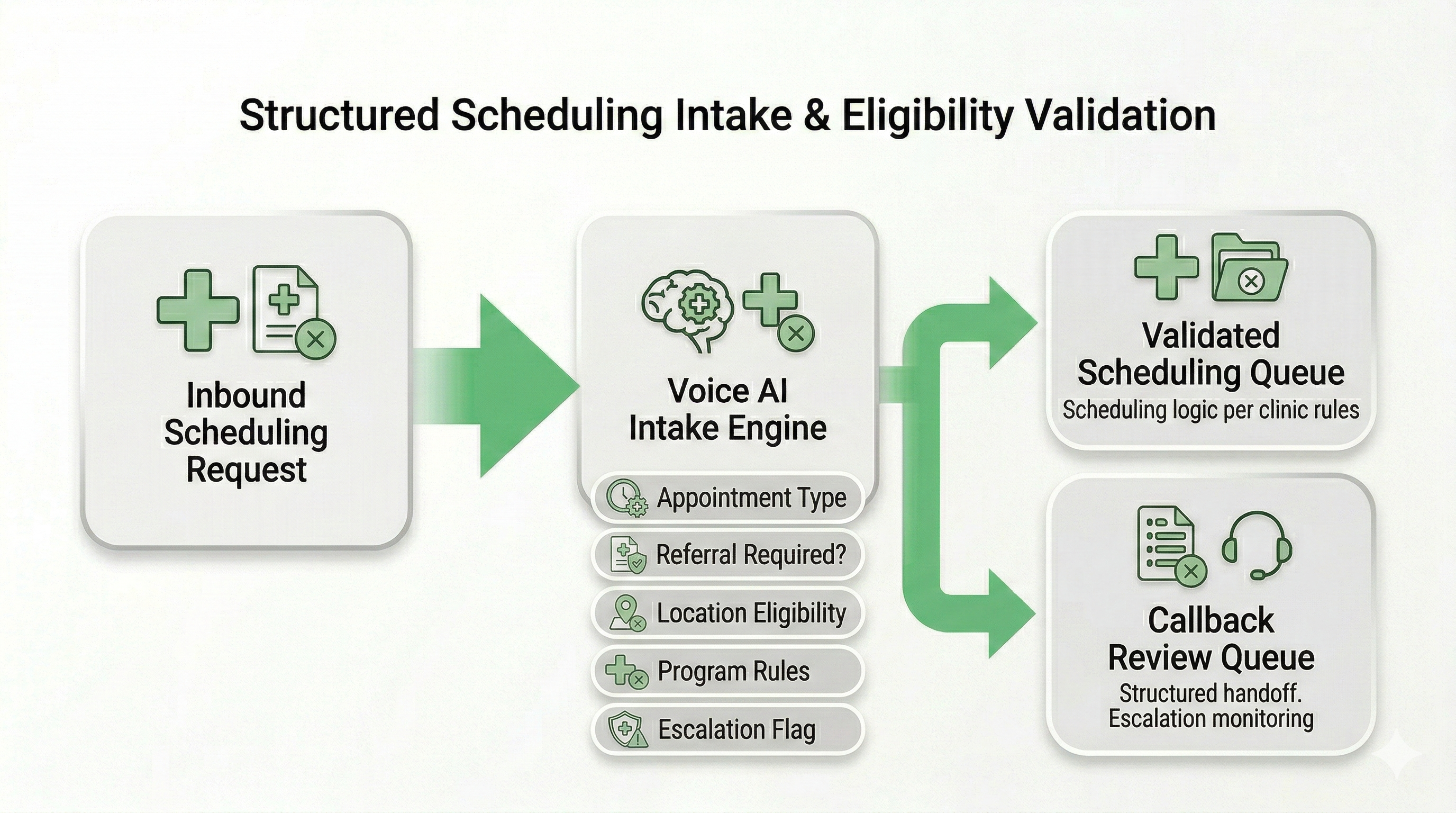
Structured Intake & Eligibility Pre-Screening — Reduce Rework Before Human Scheduling
Centralized healthcare scheduling centers often spend significant time correcting incomplete requests — missing referral details, wrong appointment types, incomplete patient information, or bookings that fail eligibility checks.
Peak Demand builds Voice AI intake workflows that gather structured, policy-aligned information before a request reaches your scheduling team. This reduces manual rework, prevents invalid bookings, and improves queue cleanliness.
Structured intake capabilities
- Appointment type confirmation: new consult, follow-up, imaging, procedure.
- Referral verification: confirm referral exists and required documentation is available.
- Program eligibility logic: enforce clinic-specific requirements.
- Location validation: confirm appropriate regional site.
- Callback structuring: create clean task queues when staff review is required.
Operational impact for scheduling teams
- Fewer incomplete bookings entering the queue.
- Reduced handle time for live schedulers.
- Lower transfer rates between departments.
- Improved referral integrity across service lines.
- More predictable intake flow during peak volume periods.
{
"section": "Structured Intake & Eligibility Pre-Screening",
"entity": "Peak Demand",
"service": "Voice AI for centralized healthcare scheduling",
"core_functions": [
"appointment classification",
"referral verification",
"program eligibility enforcement",
"location validation",
"structured callback queue creation"
],
"outcomes": [
"reduced scheduling rework",
"cleaner queues",
"lower handle time",
"improved booking integrity"
]
}
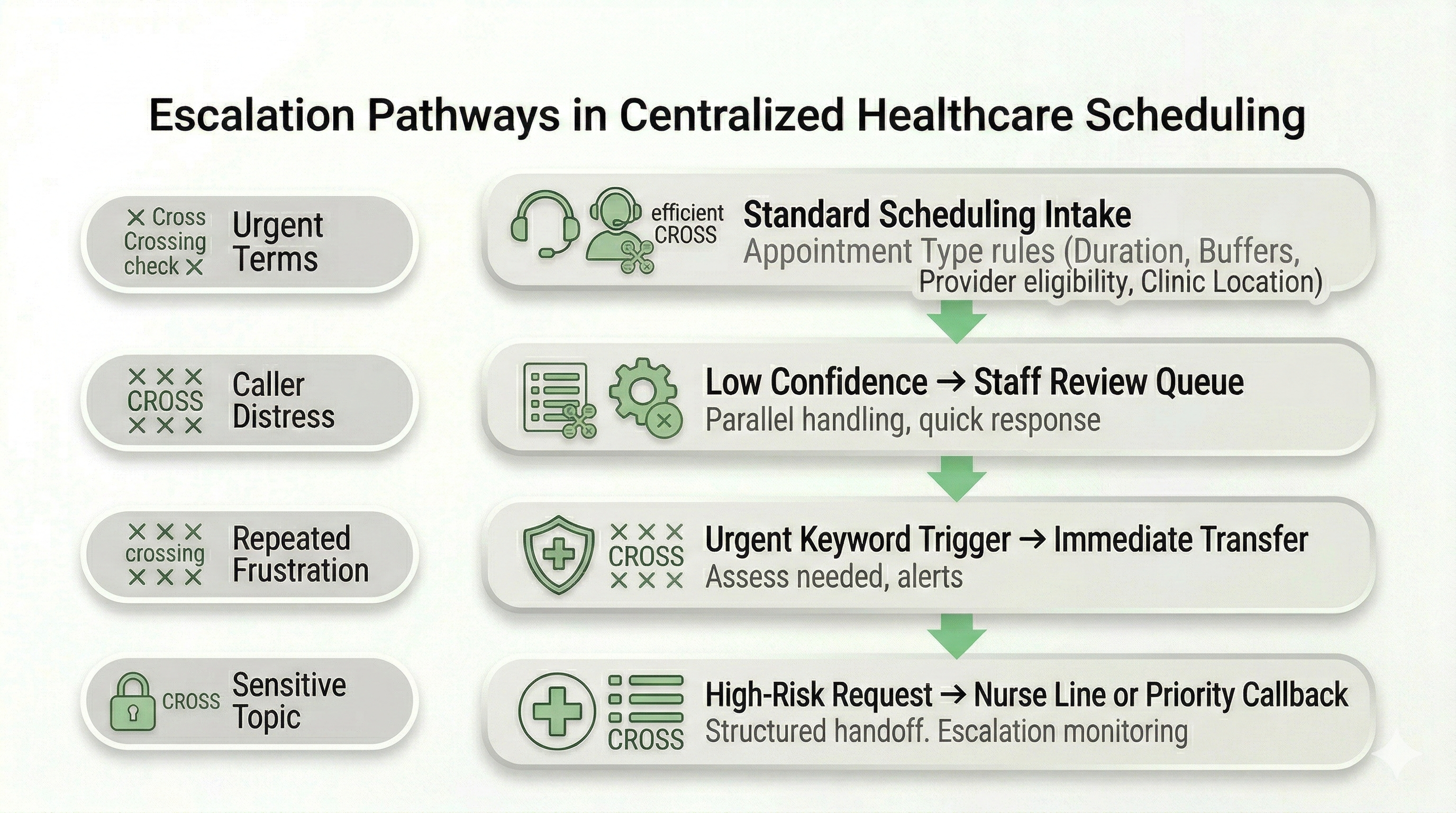
Escalation Pathways for Urgent & High-Risk Requests — Human-First When It Matters
A centralized scheduling center should never “trap” urgent callers inside automation. Scheduling workflows must support clear human override paths and policy-driven escalation for high-risk language, safety concerns, or low-confidence interactions.
Peak Demand designs Voice AI scheduling systems with structured escalation ladders: immediate transfer options, defined nurse line routing (when applicable), and staff callbacks with priority tagging — based on the thresholds your clinical leadership approves.
Escalation triggers (policy-driven)
- Urgent symptom keywords: triggers immediate human routing where configured.
- Repeated frustration: caller dissatisfaction routed to staff without delay.
- Low-confidence detection: uncertain intent → transfer or priority callback.
- Sensitive topics: defined categories routed to approved human pathways.
- Hard stop boundaries: the AI avoids unapproved clinical guidance.
Escalation pathways we implement
- Immediate transfer: to live scheduling, switchboard, or designated queue.
- Nurse line routing: when your organization has approved pathways.
- Priority callback creation: structured task with urgency tag and summary.
- Human override options: “speak to staff” / “press 0” / escalation phrase triggers.
- Escalation logging: reasons captured for governance and workflow tuning.
What happens if a caller sounds urgent or uses emergency language?
Can we add a “human override” option at any time?
Does the AI provide clinical advice?
{
"section": "Escalation Pathways for Centralized Scheduling",
"entity": "Peak Demand",
"service": "Voice AI for healthcare scheduling centers",
"safety_controls": [
"policy-driven escalation triggers",
"human override pathways",
"low-confidence routing",
"urgent keyword detection",
"escalation logging"
],
"pathways": [
"immediate transfer",
"nurse line routing (where applicable)",
"priority callback creation",
"staff review queue"
],
"positioning": "human-first when it matters"
}
Integrations for Centralized Scheduling — Systems of Record, Queues, and Notifications (Scoped + Reviewable)
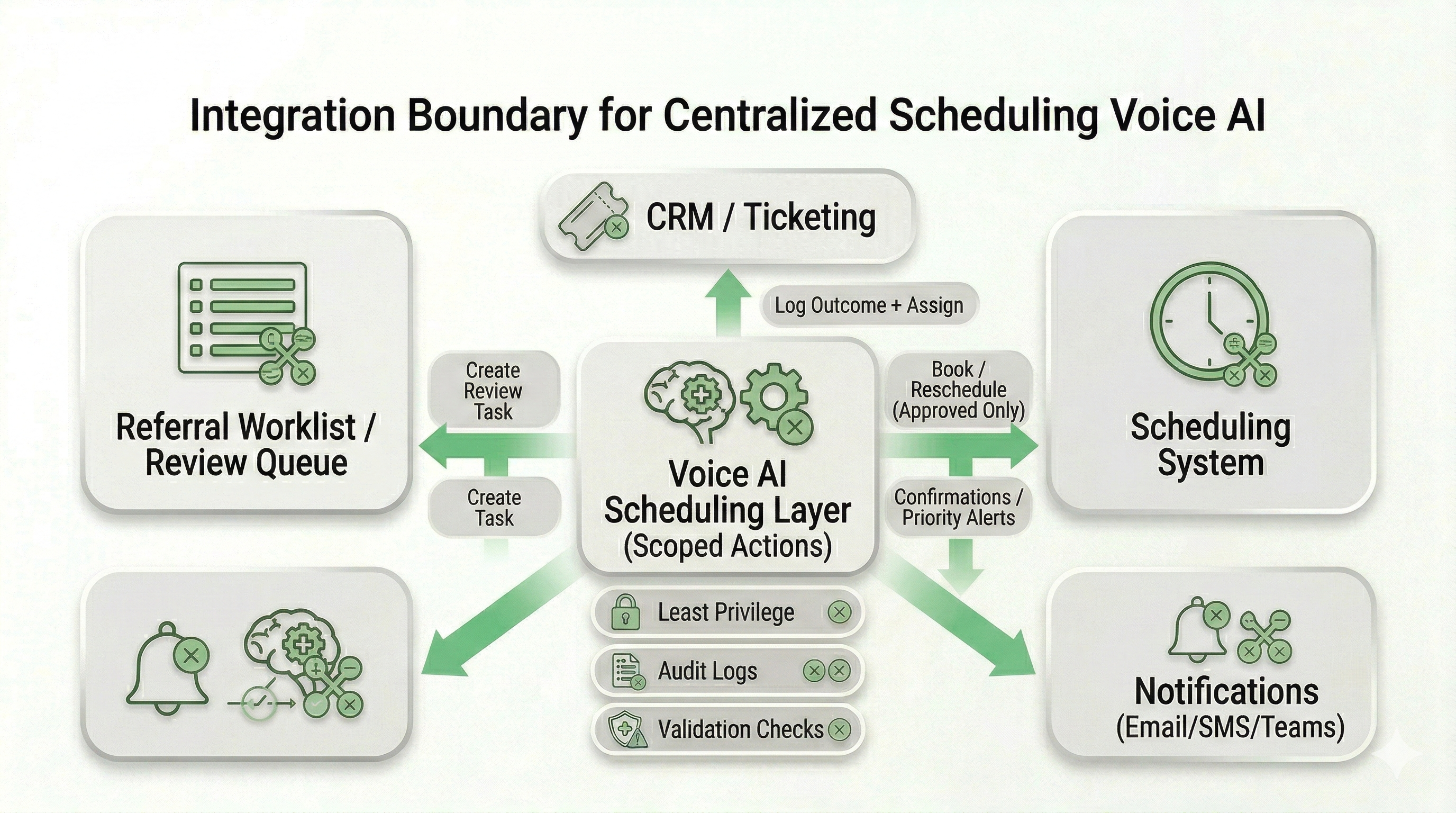
A centralized healthcare scheduling center becomes more reliable when routing decisions and intake outcomes can be written into the systems your teams already use — scheduling platforms, referral worklists, CRM/ticketing queues, and internal notifications. The goal is task completion without broad system access.
Peak Demand implements least-privilege integration patterns so Voice AI can perform only the actions you approve: create a callback task, attach an intake summary, route to a queue, send a confirmation, or book into an approved schedule — with audit visibility.
What centralized scheduling centers commonly connect
- Scheduling platforms: appointment creation, reschedule, cancellation, waitlist workflows.
- Referral worklists: referral status checks, prerequisite tracking, staff review queues.
- CRM / ticketing: structured tasks, call outcomes, assignment to teams or service lines.
- Internal notifications: email/SMS/Teams/Slack alerts for priority callbacks or escalations.
- Call center queues: transfers to appropriate teams with context attached.
How we keep integrations secure and reviewable
- Scoped permissions: read/write separation and narrow access by workflow.
- Token-based auth: OAuth/OIDC where supported; scoped service tokens otherwise.
- Action logging: track calendar writes, queue transfers, task creation, and admin changes.
- Validation checks: confirm required fields before a booking/task is finalized.
- Environment separation: staging vs production to reduce deployment risk.
{
"section": "Centralized Scheduling Integrations",
"entity": "Peak Demand",
"service": "Voice AI for centralized healthcare scheduling centers",
"connected_systems": [
"scheduling platforms",
"referral worklists / staff review queues",
"CRM / ticketing systems",
"call center queues",
"internal notification tools"
],
"security_controls": [
"least-privilege scopes",
"OAuth/OIDC or scoped service tokens",
"action logging and auditability",
"validation checks before writes",
"staging vs production separation"
],
"outcomes": [
"task completion without broad access",
"cleaner queues",
"faster routing",
"reviewable governance posture"
]
}
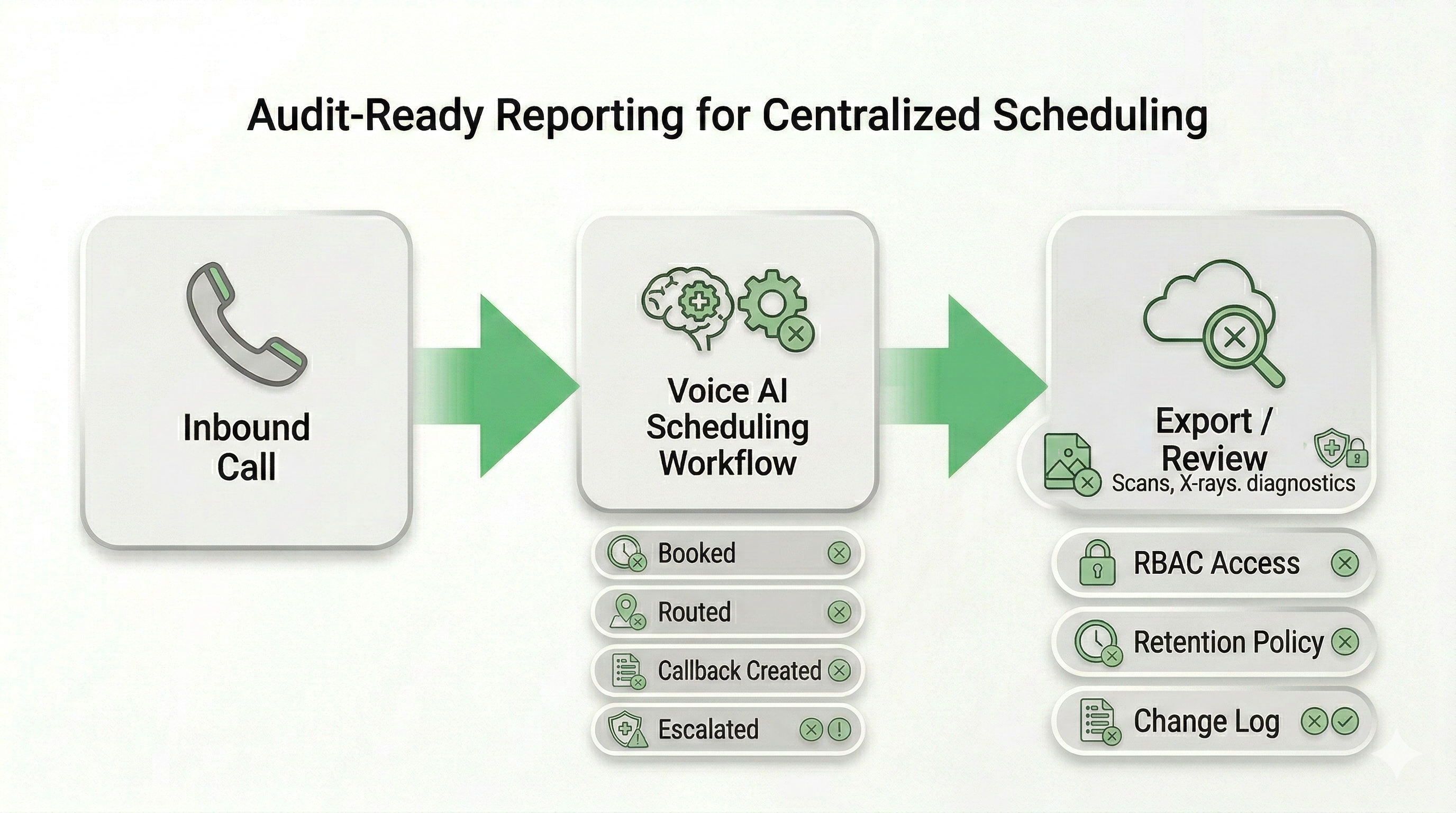
Audit-Ready Reporting for Centralized Scheduling — Outcomes, Escalations, and Queue Integrity
Regional scheduling centers need visibility and governance — not a black box. If a call is routed incorrectly, a referral is missing prerequisites, or an escalation is triggered, your team should be able to trace what happened, why it happened, and what action was taken.
Peak Demand configures Voice AI scheduling deployments with policy-driven reporting — from metadata-only logs to structured summaries and controlled transcript retention where required. The emphasis is reviewability for operations, privacy, and IT/security stakeholders.
What your team can review (configurable)
- Call outcomes: booked, routed, transferred, callback created, review queued.
- Routing evidence: service line selected, location chosen, eligibility checks applied.
- Escalation reasons: urgent keyword triggers, low confidence, “speak to staff” requests.
- System actions: calendar writes, task creation, notification events (where integrated).
- QA sampling support: review queues to validate workflow quality over time.
Governance controls we support
- RBAC access model: restrict who can view/export logs or summaries.
- Retention posture: configurable retention windows aligned to your policy.
- Minimization options: reduce captured content to what’s needed for scheduling.
- Exportability: structured exports for review, vendor due diligence, or investigations.
- Change logging: track workflow edits and admin changes over time.
Can we get a record of every call outcome without storing transcripts?
Can our security or privacy team audit what the Voice AI did?
Do you log workflow changes over time?
{
"section": "Audit-Ready Reporting for Centralized Scheduling",
"entity": "Peak Demand",
"service": "Voice AI for centralized healthcare scheduling centers",
"reporting_outputs": [
"call outcomes (booked, routed, transferred, callback created)",
"routing evidence (service line, location, eligibility checks)",
"escalation reasons (urgent keywords, low confidence, human override)",
"system action logs (writes, tasks, notifications where integrated)",
"QA review queues (policy-driven)"
],
"governance_controls": [
"role-based access control (RBAC)",
"retention windows and deletion posture",
"minimization options",
"exportable records",
"change logging for workflows"
],
"positioning": "reviewable oversight for operations + privacy + IT/security"
}
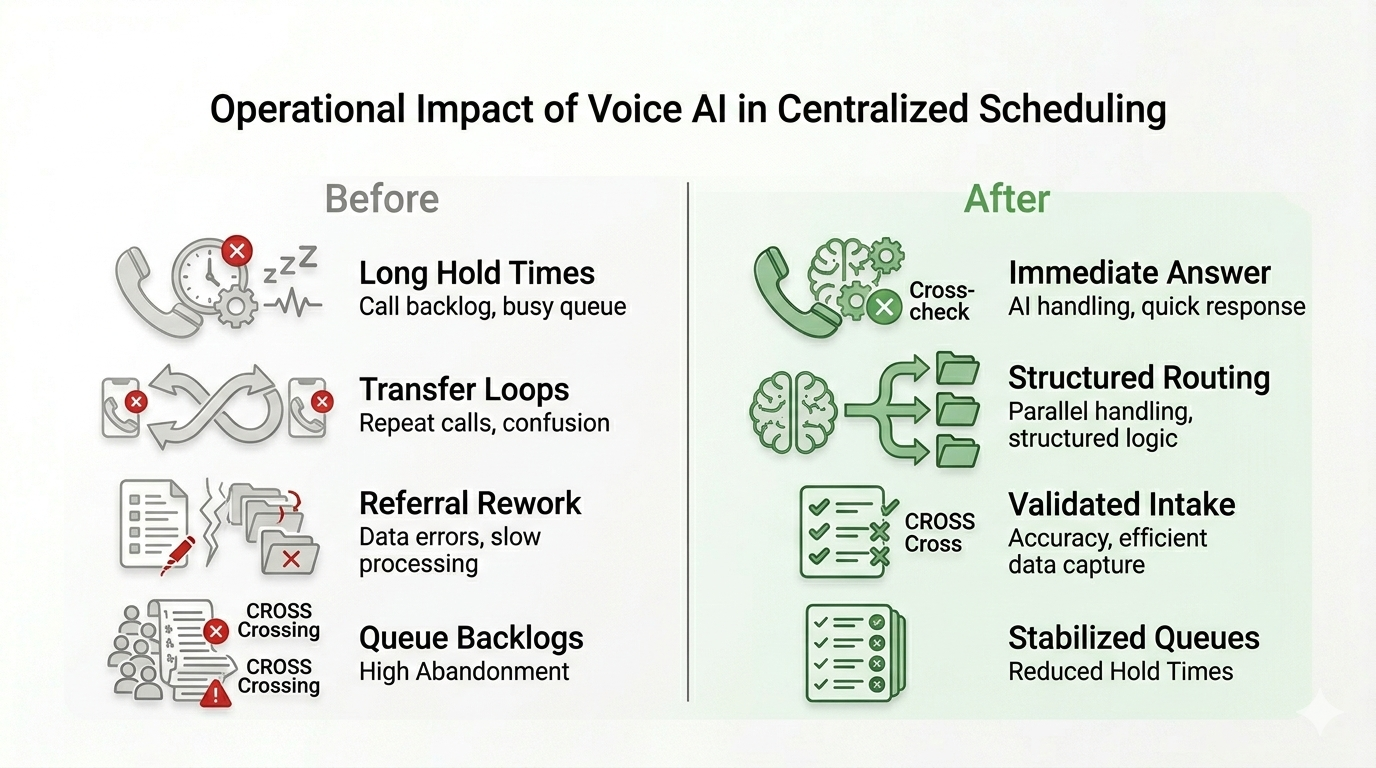
Operational ROI for Centralized Healthcare Scheduling Centers
Centralized scheduling centers exist to create order across a distributed healthcare network. When routing is inconsistent or queues become unstable, downstream clinical operations are affected.
Voice AI introduces a parallel intake and classification layer that absorbs demand spikes, reduces unnecessary transfers, and ensures requests enter the correct workflow before human intervention is required.
Operational Gains
- Reduced call abandonment: immediate answer rate during peak volume.
- Lower average handle time: structured intake before staff engagement.
- Fewer transfer loops: routing accuracy improves first-touch resolution.
- Cleaner referral workflows: incomplete requests flagged before queue entry.
- After-hours capture: no lost scheduling demand outside business hours.
Network-Level Benefits
- Queue stabilization: smoother demand distribution across regional sites.
- Improved booking velocity: fewer back-and-forth interactions.
- Better resource allocation: staff focus on complex cases, not routing errors.
- Scalable intake model: supports expansion to new clinics or specialties.
- Measurable oversight: track outcomes and escalation patterns over time.
{
"section": "Operational ROI for Centralized Scheduling",
"entity": "Peak Demand",
"service": "Voice AI healthcare scheduling center automation",
"operational_outcomes": [
"reduced abandonment",
"lower handle time",
"fewer transfer loops",
"queue stabilization",
"after-hours capture"
],
"network_benefits": [
"scalable intake layer",
"resource optimization",
"improved booking velocity",
"measurable oversight"
],
"positioning": "enterprise-grade operational lift without governance compromise"
}
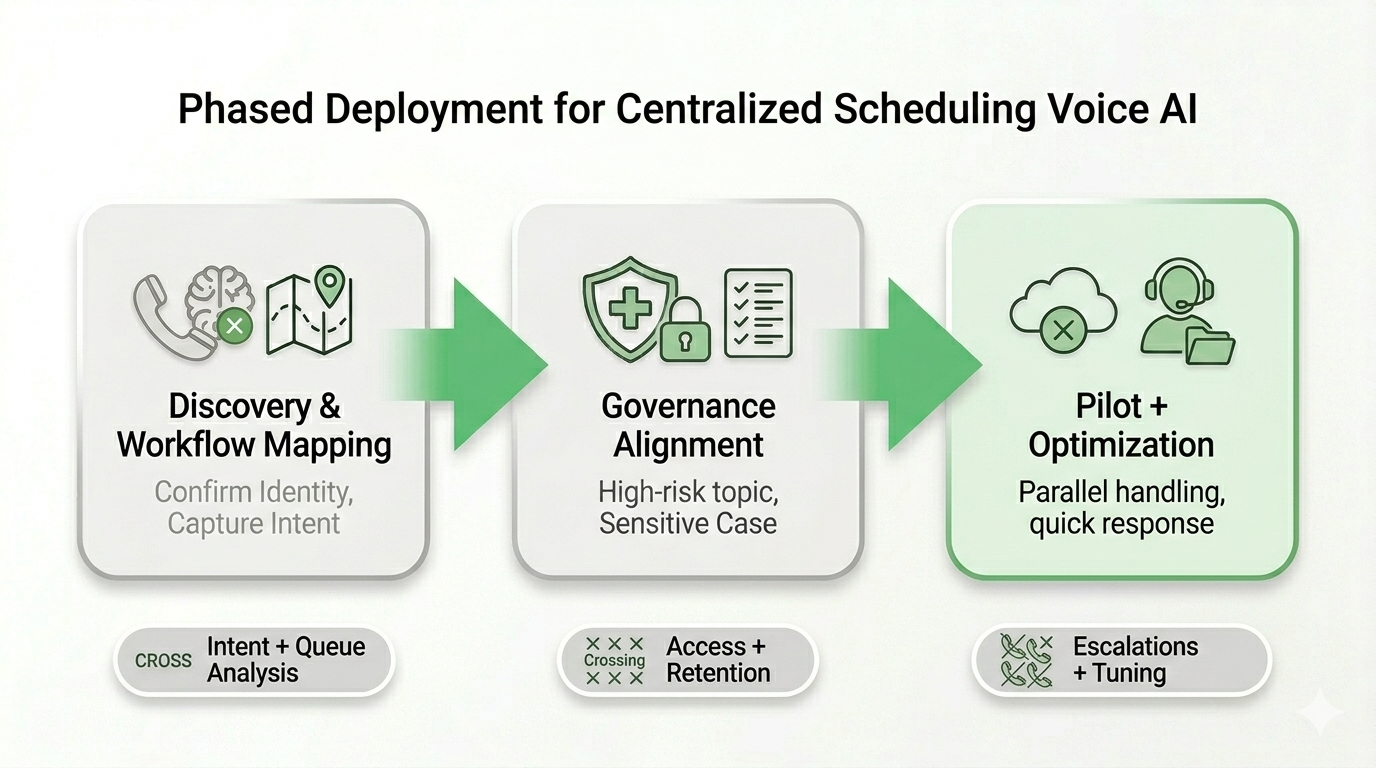
Enterprise Deployment Model — Phased Rollout Across Regional Scheduling Networks
Centralized scheduling is a high-dependency operational layer. That means deployment needs to be staged, measurable, and reversible — not a “big bang” cutover.
Peak Demand delivers fully managed Voice AI scheduling deployments using a phased model: discovery, governance alignment, pilot rollout, and optimization — with escalation monitoring and workflow tuning as real-world call patterns emerge.
How the rollout is staged (practical)
- Start with 1–2 call types: high-volume scheduling requests or a defined service line.
- Limit scope intentionally: approved workflows only, no uncontrolled expansion.
- Test with real scenarios: referral prerequisites, eligibility rules, transfers, and callbacks.
- Use safe fallback: human override and priority escalation from day one.
- Expand by confidence: add more specialties, locations, or workflows as stability proves out.
What leadership teams get during rollout
- Workflow documentation: routing maps and intake logic in reviewable form.
- Governance posture: access model, logging plan, retention approach.
- Escalation reporting: what triggered escalation and how it was handled.
- Operational feedback loop: tune workflows based on queue performance.
- Expansion plan: a clear roadmap for multi-location rollout.
Can we pilot this with one hospital site or one service line first?
Do we have to replace our phone system to deploy Voice AI?
How do you prevent scope creep once the pilot starts working?
{
"section": "Enterprise Deployment Model for Centralized Scheduling",
"entity": "Peak Demand",
"service": "Voice AI for centralized healthcare scheduling",
"deployment_phases": [
"discovery and workflow mapping",
"governance and security alignment",
"pilot rollout and optimization"
],
"rollout_principles": [
"start narrow with defined call types",
"human override and escalation from day one",
"test real scenarios before expansion",
"expand by confidence and governance approval"
],
"positioning": "fully managed, staged rollout for high-dependency operations"
}
Why Peak Demand for Enterprise Healthcare Scheduling Networks
Centralized healthcare scheduling is not a consumer call flow problem. It is an operational stability layer that affects referral velocity, provider utilization, patient access, and compliance posture.
Peak Demand designs fully managed, custom Voice AI routing systems for healthcare organizations that require governance visibility, escalation control, and integration precision — not generic SaaS call trees.
What differentiates our approach
- Custom workflow engineering: built around your referral, scheduling, and routing logic.
- Policy-driven escalation design: human override pathways defined before deployment.
- Integration scoping: limited-permission connections to approved scheduling systems.
- Audit-ready logging posture: traceable outcomes and escalation documentation.
- Phased rollout methodology: controlled pilot expansion across regions.
Who we typically work with
- Regional hospital networks centralizing specialty intake.
- Enterprise outpatient groups consolidating referral management.
- Provincial or multi-site systems stabilizing queue performance.
- Operations leadership teams responsible for measurable booking velocity.
- IT & compliance stakeholders requiring governance review before launch.
{
"section": "Why Peak Demand for Centralized Healthcare Scheduling",
"entity": "Peak Demand",
"service": "Enterprise Voice AI scheduling and routing",
"differentiation": [
"custom workflow engineering",
"policy-driven escalation logic",
"integration scoping with least privilege",
"audit-ready logging",
"phased enterprise rollout"
],
"target_stakeholders": [
"operations leadership",
"IT and compliance teams",
"regional hospital networks",
"multi-site outpatient systems"
],
"positioning": "fully managed enterprise healthcare voice AI partner"
}
Ready to Stabilize Centralized Scheduling Across a Multi-Location Healthcare Network?
If your scheduling center is managing high call volume, complex routing between sites and service lines, and referral prerequisites that create constant rework, Peak Demand can design a custom-built, fully managed Voice AI routing + scheduling layer engineered for enterprise healthcare operations.
We implement Voice AI with a phased rollout model: define workflows, align governance controls, pilot safely, then expand by confidence — with escalation monitoring and audit-ready reporting configured to your requirements.
What we’ll review on a Discovery Call
- Network routing reality: sites, service lines, specialties, and transfer rules.
- Top call types: scheduling, referral follow-up, prerequisites, reschedules, cancellations.
- Escalation policies: urgent language, safety triggers, priority callbacks, human override.
- Queue + system touchpoints: scheduling tools, referral worklists, ticketing/CRM, notifications.
- Pilot scope plan: where to start small and expand without disrupting operations.
For Operations, IT & Compliance Stakeholders
- Workflow documentation: reviewable routing maps + intake logic.
- Access model overview: RBAC and least-privilege integration design.
- Logging posture: outcomes vs summaries vs transcripts (policy-driven).
- Retention approach: configurable retention windows aligned to your governance needs.
- Audit readiness: exportable records + change logging for workflow updates.
Toronto-based AI agency. Enterprise healthcare experience. Custom builds — not off-the-shelf call trees.
Explore Voice AI Pathways for Centralized Healthcare Scheduling Centers
Centralized healthcare scheduling teams usually begin by stabilizing high-volume booking, referral coordination, and queue management across clinics, specialty departments, imaging workflows, and regional access lines. From there, organizations often expand into broader patient intake automation, after-hours support, and more standardized access workflows across sites and service lines.
The resources below connect the main healthcare hub, the primary service entry points, adjacent patient access and scheduling models, and the governance pages most relevant to regulated healthcare communication environments in Canada and the United States.
Core Healthcare Entry Points
Patient Access and Referral Coordination
Clinic Network Scheduling and Access Workflows
{
"module": "healthcare_interlinks_scheduling_centers",
"page_context": "voice-ai-healthcare-centralized-scheduling-center",
"core_entry_points": [
"https://peakdemand.ca/healthcare-voice-ai-resource-hub",
"https://peakdemand.ca/ai-voice-receptionist-after-hours-answering-service-for-healthcare-providers-appointment-booking",
"https://peakdemand.ca/voice-ai-healthcare-call-center-automation"
],
"patient_access_and_referral_coordination": [
"https://peakdemand.ca/voice-ai-specialty-clinics-outpatient-networks",
"https://peakdemand.ca/voice-ai-for-medical-imaging-diagnostics-scheduling",
"https://peakdemand.ca/voice-ai-hospital-call-routing-multi-location-networks"
],
"clinic_network_scheduling_and_access_workflows": [
"https://peakdemand.ca/ai-receptionist-medical-clinic-canada",
"https://peakdemand.ca/voice-ai-family-medicine-clinics-patient-intake-appointment-scheduling-prescription-requests-after-hours",
"https://peakdemand.ca/voice-ai-for-womens-health-clinics-screening-centres"
],
"governance_and_compliance": [
"https://peakdemand.ca/phipa-compliant-ai-voice-receptionist-ontario-clinics",
"https://peakdemand.ca/hipaa-compliant-voice-ai-receptionist-healthcare",
"https://peakdemand.ca/enterprise-voice-ai-compliance-certifications-rfp-vendor-ccai-customer-service-healthcare-utilities-government-canadian-ai-agency"
],
"intent": "Centralized scheduling internal linking + pathway clustering + LLM surfacing + crawl reinforcement"
}
Regulatory & Governance Framework References (Canada & United States)
Centralized healthcare scheduling centers may operate within regulated privacy and security environments. The following legislation and regulatory bodies inform how enterprise Voice AI deployments are structured, reviewed, and governed across hospital networks and multi-location healthcare systems.
Canada
Regulatory applicability varies depending on jurisdiction, organizational structure, and data handling model. Voice AI deployments for centralized scheduling can be configured with structured access controls, escalation pathways, logging posture, and retention policies that support internal governance review prior to go-live.
{
"section": "Healthcare Regulatory & Governance References",
"entity": "Peak Demand",
"geo": ["Canada", "United States"],
"regulatory_sources": [
"PHIPA",
"PIPEDA",
"Information and Privacy Commissioner of Ontario",
"Office of the Privacy Commissioner of Canada",
"HIPAA",
"HITECH",
"NIST Cybersecurity Framework"
],
"purpose": "Provide authoritative legislative and governance context for enterprise Voice AI scheduling deployments"
}
Explore your own AI use case on a discovery call.
