
Voice AI for Public Sector Health Systems & Regional Booking Lines

Provincial and state health systems face unique pressures: centralized booking backlogs, seasonal surges, policy-driven intake rules, and public accountability. Off-the-shelf IVR tools rarely meet governance, privacy, and procurement expectations.
Peak Demand delivers fully managed, custom-built Voice AI deployments for public sector health environments across Canada, with U.S. alignment where applicable. Workflows are designed to support policy-aligned routing, least-privilege integration, audit visibility, and safe escalation — not just automation for automation’s sake.
For the broader service overview (Canada + U.S., HIPAA/PIPEDA/PHIPA context), see:
https://peakdemand.ca/ai-voice-receptionist-after-hours-answering-service-for-healthcare-providers-appointment-booking
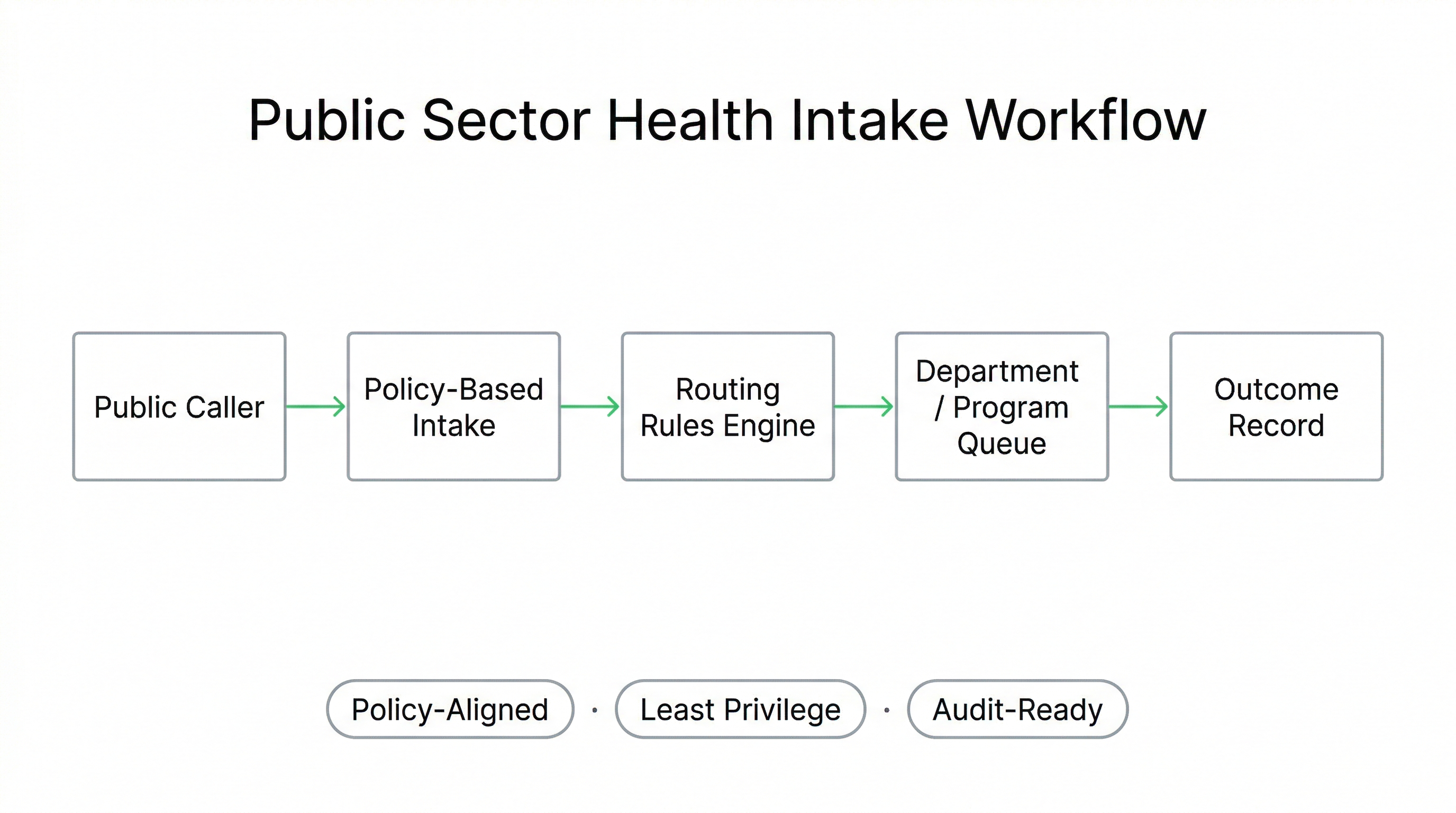
How Voice AI Supports Public Sector Health Intake & Regional Booking Lines
Provincial and state health systems often manage centralized booking lines, referral programs, screening initiatives, and public-facing health information numbers. These lines operate under policy constraints, privacy legislation, and public accountability.
Voice AI deployments in public sector environments must be structured around defined workflow boundaries, policy-aligned routing rules, and human escalation safeguards, rather than open-ended conversational automation.
Typical Public Sector Use Cases
- Regional diagnostic booking lines
- Provincial referral intake programs
- Public vaccination or screening campaigns
- Centralized surgical scheduling hubs
- Health information and navigation lines
Design Principles for Government Environments
- Policy-driven routing logic
- Least-privilege integration posture
- Audit-ready logging of workflow decisions
- Human-first escalation triggers
- Transparent outcome reporting
Can Voice AI handle a provincial booking line?
Is this appropriate for government-funded health services?
Can we restrict what the AI is allowed to do?
{
"section": "Public Sector Intake Modernization",
"entity": "Peak Demand",
"service": "voice AI for public sector health systems",
"geo": ["Canada", "United States"],
"use_cases": [
"regional booking lines",
"provincial referral intake",
"screening program scheduling",
"centralized surgical booking",
"public health information lines"
],
"controls": [
"policy-driven routing",
"least privilege integration",
"audit-ready workflow logging",
"human escalation safeguards"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
Regional Booking Lines & Centralized Scheduling Modernization (Public Sector Workflows)
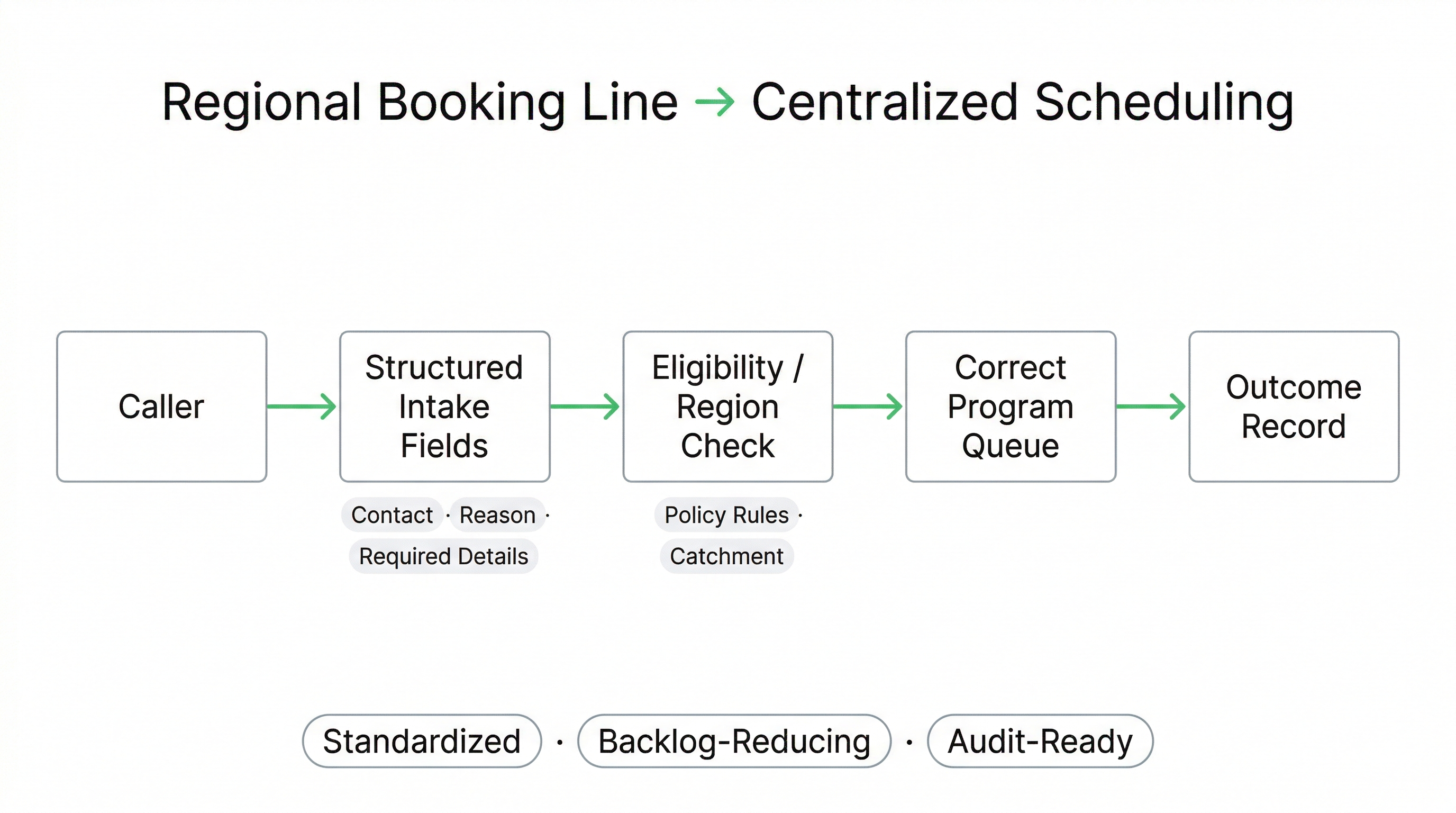
Regional booking lines and centralized scheduling centres must handle high call volume while enforcing program eligibility rules, jurisdictional boundaries, modality-specific requirements (e.g., imaging), and standardized intake fields. When intake data is incomplete, patients call repeatedly and staff spend time in “missing-info loops.”
Voice AI can be configured to capture required intake fields first, validate basic routing criteria, and either route the caller into the correct program queue or escalate to staff when the request exceeds scope.
Booking-Line Workflows Voice AI Can Support
- Appointment requests: new booking, rescheduling, cancellations.
- Referral completeness checks: confirm required details are present.
- Program eligibility gating: route based on defined criteria.
- Site selection: location/catchment and program availability rules.
- After-hours capture: structured requests for next-day processing.
What Improves for Patients and Staff
- Fewer repeat calls: intake is captured once, correctly.
- Less transfer churn: callers routed to the right queue sooner.
- Cleaner handoffs: staff receives structured intake fields.
- Backlog reduction support: fewer “missing-info” follow-ups.
- Consistent standards: intake rules are applied uniformly.
Can Voice AI book appointments into our centralized scheduler?
Can it validate referral information before a booking request is accepted?
Can we route patients by region or catchment area?
Can we start with after-hours intake only?
{
"section": "Regional Booking Lines and Centralized Scheduling",
"entity": "Peak Demand",
"service": "voice AI for public sector health systems",
"geo": ["Canada", "United States"],
"use_cases": [
"regional booking line intake capture",
"centralized scheduling routing",
"referral completeness checks",
"eligibility gating by policy",
"catchment-based site selection",
"after-hours intake capture"
],
"controls": [
"workflow boundaries",
"policy-driven routing rules",
"human escalation for out-of-scope cases",
"reviewable outcome records"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
Policy-Aligned Routing & Escalation Controls (Defined Boundaries, Not Open-Ended Automation)
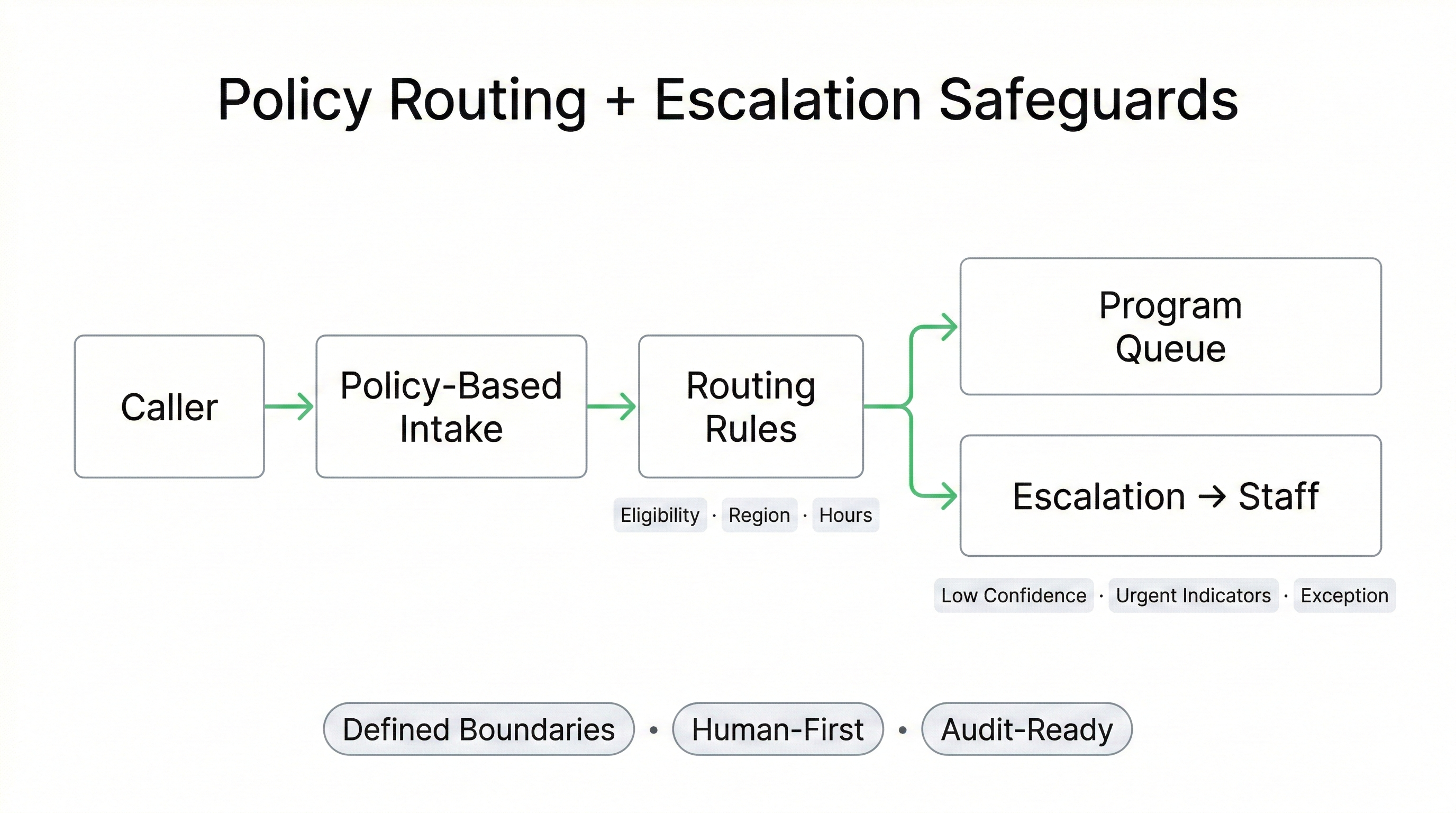
Public sector health lines must follow program rules, jurisdiction boundaries, and operational policies. Routing cannot depend on ad-hoc scripts or agent interpretation. Workflows must be defined, testable, and aligned with how the health authority expects intake to be handled.
Voice AI can be configured to enforce policy-based routing with clearly defined escalation triggers. When a caller request exceeds the allowed scope, the workflow escalates to staff rather than improvising.
Policy-Aligned Routing Rules (Examples)
- Program eligibility: route by defined inclusion criteria (as configured).
- Jurisdiction and catchment: route by region, site coverage, or service boundaries.
- Service-line routing: bookings, referrals, screening, general navigation.
- Hours-aware handling: live queue vs after-hours capture rules.
- Standard intake fields: require key details before queue placement.
Escalation Triggers (Human-First Safeguards)
- Low confidence: intent unclear or information incomplete.
- Urgency indicators: escalation pathways for sensitive scenarios.
- Repeated frustration: caller cannot progress through intake.
- Out-of-scope requests: policy exception or uncommon case.
- Integration restrictions: action not permitted under scope.
Can we control what the Voice AI is allowed to say and do?
What happens when the caller doesn’t fit the program rules?
Can the system transfer to a human when it’s not sure?
Can policy teams review routing rules before launch?
{
"section": "Policy-Aligned Routing and Escalation Controls",
"entity": "Peak Demand",
"service": "voice AI for public sector health systems",
"geo": ["Canada", "United States"],
"use_cases": [
"policy-based routing to program queues",
"catchment and jurisdiction routing",
"hours-aware live vs after-hours handling",
"standard intake field capture",
"exception handling via escalation"
],
"controls": [
"defined workflow boundaries",
"low-confidence escalation thresholds",
"urgent indicator escalation pathways",
"reviewable routing logic",
"human-first exception handling"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
Surge Capacity & Public Health Event Response (Overflow Capture Without Unsafe Automation)
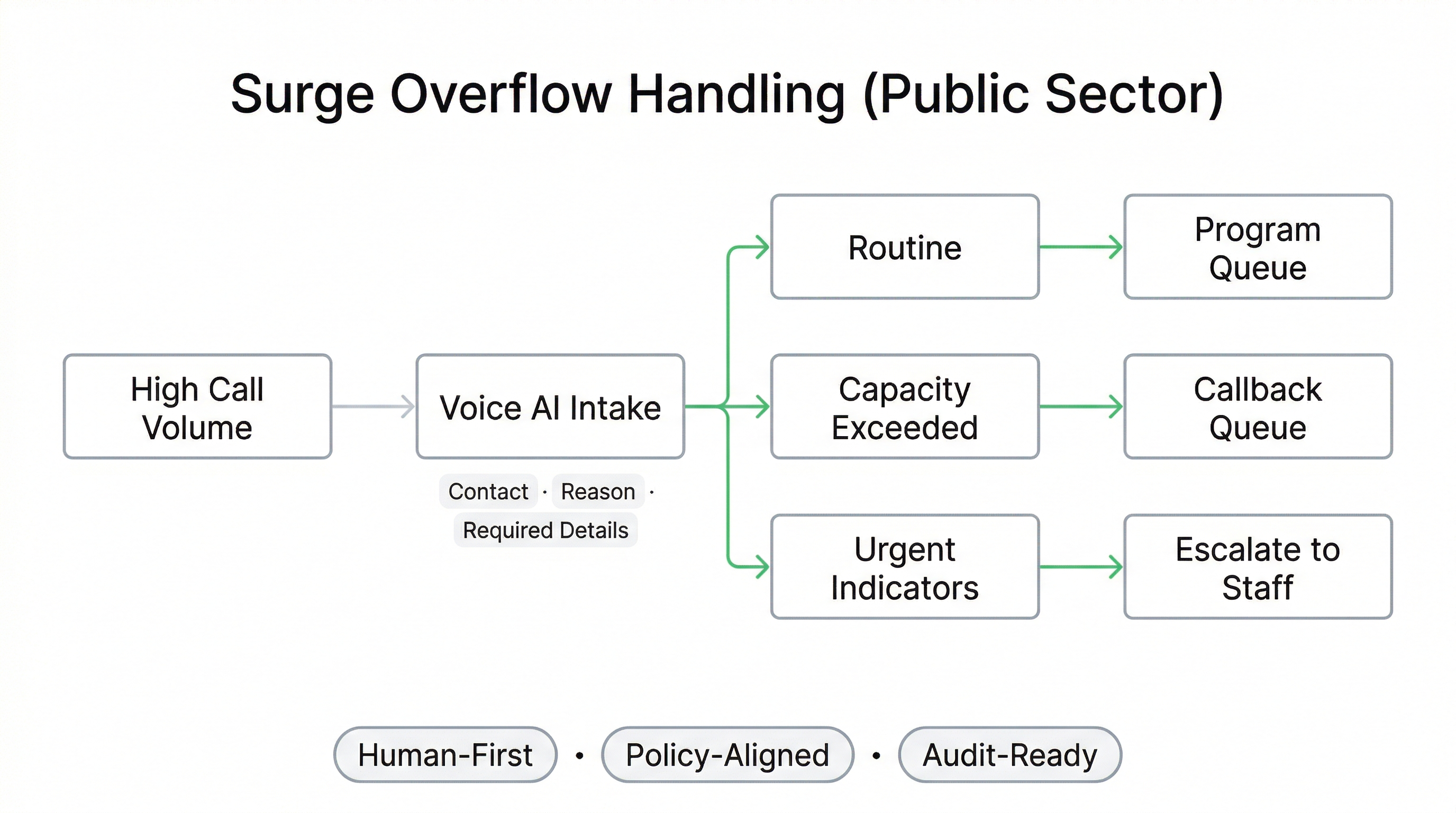
Public sector health lines experience predictable and unpredictable surges: seasonal illness cycles, service disruptions, facility closures, program launches, and public health events. Traditional IVR trees and human queues can break under load, resulting in abandoned calls and repeated dialing.
Voice AI can be configured to support surge overflow capture by collecting structured intake, routing to the correct program queues, and escalating to staff when urgency, uncertainty, or exception scenarios are detected. The goal is capacity smoothing and clarity — not replacing clinical judgement.
Surge Handling Patterns (Public Sector)
- Overflow intake: capture requests instead of losing calls to abandonment.
- Callback queue creation: structured follow-up lists for staff teams.
- Program-based triage: route by defined policy criteria and service lines.
- Hours-aware handling: live queue vs after-hours intake capture.
- Service disruption messaging: policy-approved updates (as configured).
Human-First Safety Boundaries
- Urgency indicators: triggers that force escalation to staff.
- Low-confidence escalation: transfer when intent is unclear.
- Exception handling: escalate when policy rules don’t apply.
- No clinical diagnosis scope: intake and routing, not medical decision-making.
- Reviewable outcomes: surge performance can be assessed post-event.
Can Voice AI handle surge volume on a public health line?
What happens if a caller sounds urgent?
Can we add temporary workflows during a public health event?
Does this replace nurses or clinical triage?
{
"section": "Surge Capacity and Public Health Event Response",
"entity": "Peak Demand",
"service": "voice AI for public sector health systems",
"geo": ["Canada", "United States"],
"use_cases": [
"surge overflow intake capture",
"callback queue creation",
"event-specific routing and messaging (policy-approved)",
"hours-aware after-hours intake capture",
"urgent escalation to staff"
],
"controls": [
"human-first escalation boundaries",
"low-confidence escalation",
"no clinical diagnosis scope",
"reviewable outcome records",
"change governance for event updates"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
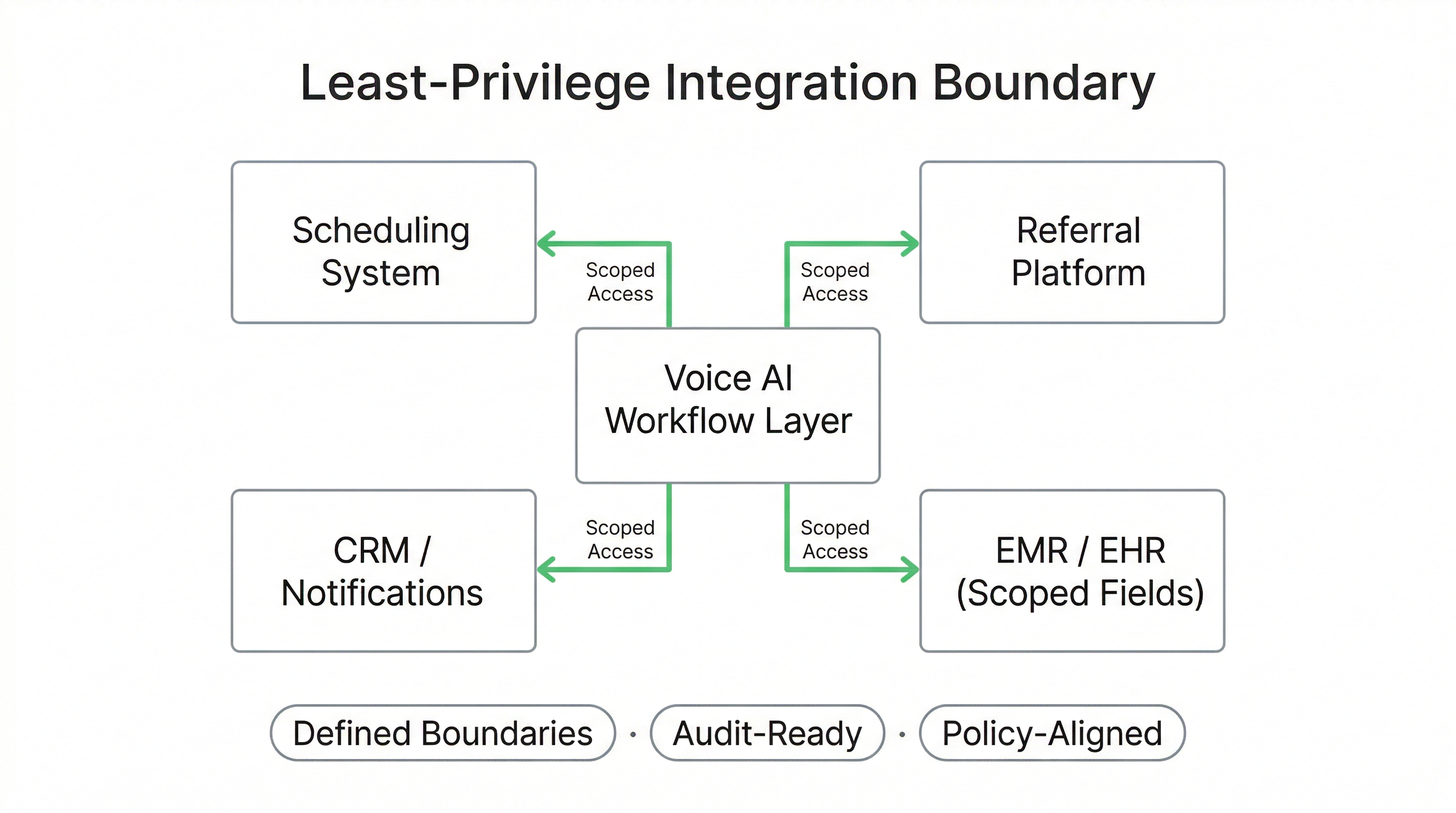
Integration Boundaries & Least-Privilege Architecture (Public Sector Ready)
Public health systems often operate complex environments: centralized schedulers, referral management tools, EMR/EHR platforms, CRM systems, and telephony infrastructure. Integration must be carefully scoped to avoid unnecessary exposure of sensitive data.
Voice AI deployments are structured around a least-privilege integration posture — meaning access is limited to defined fields, allowed actions, and documented workflow boundaries.
Integration Design Principles
- Scoped permissions: access only to required data fields.
- Purpose limitation: capture and transmit only what is needed.
- Defined allowed actions: booking, routing, message creation (as configured).
- No open system access: integrations are bounded to approved endpoints.
- Change governance: integration updates reviewed before deployment.
Technical Safeguards (Configurable)
- Encryption in transit: TLS-secured communication channels.
- Role-based access control (RBAC): restrict log and transcript visibility.
- Audit-ready event logging: track workflow actions and routing decisions.
- Retention posture: configurable storage aligned with policy.
- Separation of duties: administrative access scoped by role.
Does Voice AI need full access to our scheduling or EMR system?
Can our IT team review integration boundaries before launch?
Do you log what the AI does inside our systems?
Can we start without deep system integration?
{
"section": "Integration Boundaries and Least-Privilege Architecture",
"entity": "Peak Demand",
"service": "voice AI for public sector health systems",
"geo": ["Canada", "United States"],
"integrations": [
"centralized scheduling platforms",
"referral management systems",
"EMR/EHR systems (scoped access)",
"CRM tools",
"telephony infrastructure"
],
"controls": [
"least-privilege access",
"scoped permissions",
"purpose limitation",
"RBAC",
"audit-ready event logging",
"configurable retention posture",
"change governance"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
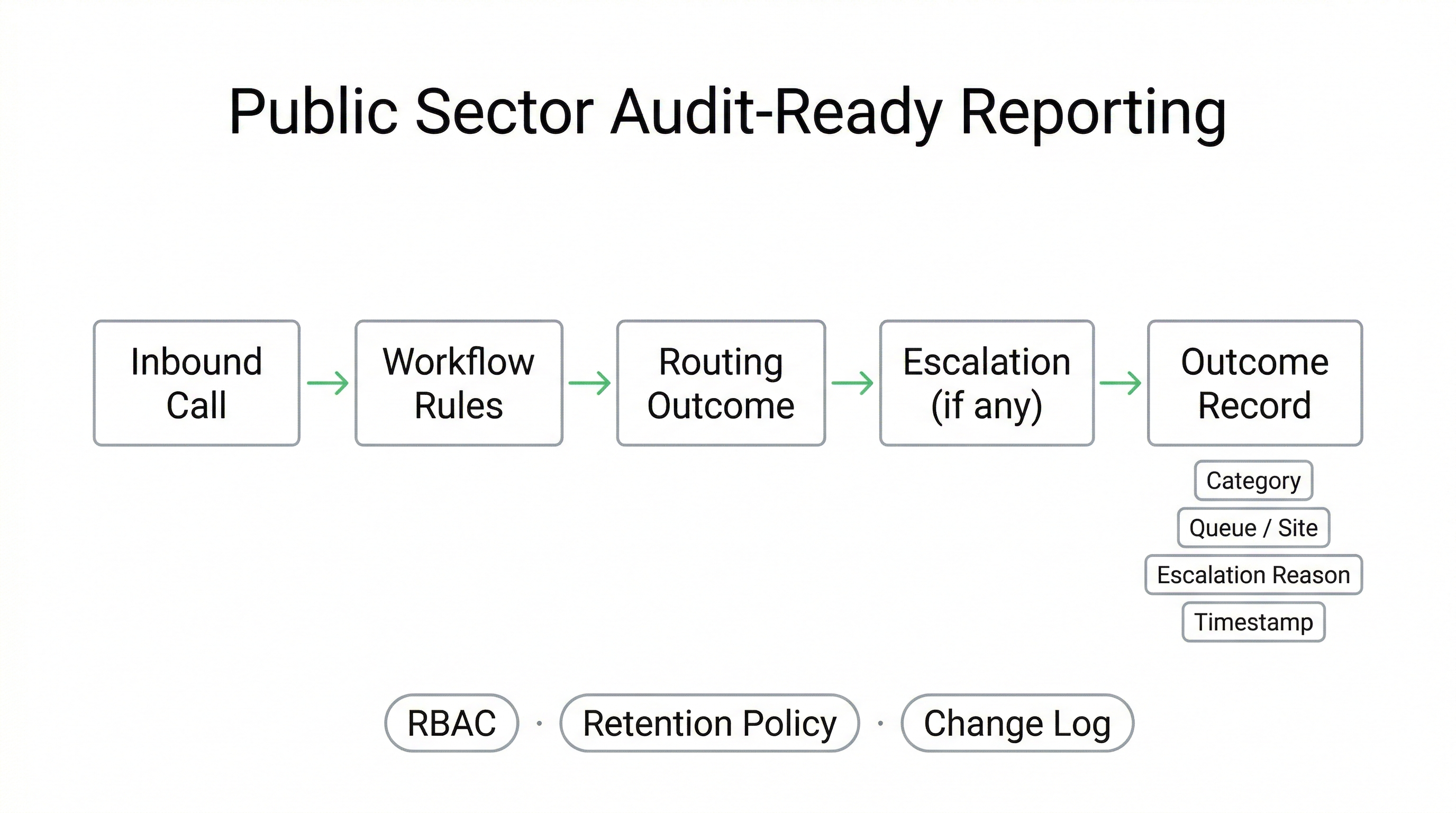
Audit Visibility & Governance Reporting (Public Accountability by Design)
Public sector health services require transparency. When intake is centralized, decision logic must be explainable, routing outcomes must be reviewable, and changes to policies or workflows should be governed. This is especially important when services span jurisdictions, programs, and multiple delivery sites.
Voice AI deployments can be structured to generate reviewable outcome records showing how a call was handled, which rules were applied, when escalation occurred, and what the final disposition was — supporting operational reporting and governance review.
Operational Reporting (Examples)
- Call categorization: booking, referral, screening, navigation, other.
- Routing outcomes: which program queue or site was selected.
- Escalation reasons: urgency, low confidence, exception cases.
- After-hours capture volume: structured requests for follow-up.
- Repeat-call reduction signals: fewer “missing-info” loops over time.
Governance & Audit Controls
- Event logs: workflow state changes and routing decisions.
- Change governance: track policy/routing updates as configured.
- RBAC: restrict access to logs and configuration tools.
- Retention posture: policy-driven storage configuration.
- Export capability: structured data for review and reporting workflows.
Can we see exactly how calls are being routed?
Can our governance team review changes to routing rules?
Can we export data for reporting to leadership?
Do you store call recordings and transcripts?
{
"section": "Audit Visibility and Governance Reporting",
"entity": "Peak Demand",
"service": "voice AI for public sector health systems",
"geo": ["Canada", "United States"],
"reporting_outputs": [
"call categorization",
"routing outcomes",
"escalation reasons",
"after-hours capture volume",
"reviewable outcome records"
],
"controls": [
"event logging",
"RBAC",
"policy-driven retention posture",
"change governance",
"structured export capability"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
PHIPA / PIPEDA / HIPAA Context for Public Health Deployments
Public sector health systems in Canada operate under PHIPA (Ontario) and other provincial privacy statutes, alongside federal legislation such as PIPEDA in certain contexts. U.S. public health entities may operate under HIPAA. Voice AI deployments in these environments must be structured around documented safeguards and governance clarity.
Compliance is not a marketing label. It is a deployment model defined by workflow boundaries, least-privilege access, audit visibility, retention posture, and human escalation safeguards.
Canadian Public Sector Context
- PHIPA (Ontario): governs personal health information handling.
- PIPEDA (Federal): applies in certain cross-jurisdictional contexts.
- Information Manager posture: defined roles and responsibilities.
- Purpose limitation: capture only what is required for intake.
- Documented safeguards: technical and administrative controls.
U.S. Public Health Context (Where Applicable)
- HIPAA Privacy Rule: safeguards for protected health information.
- HIPAA Security Rule: administrative, technical, physical safeguards.
- Business Associate posture: where applicable by relationship.
- Audit logging & access control: reviewable system actions.
- Retention configuration: aligned with organizational policy.
Are you claiming PHIPA or HIPAA certification?
Do you sign information manager or business associate agreements?
Can our privacy and compliance teams review safeguards before deployment?
Does Voice AI make clinical decisions?
{
"section": "Public Health Regulatory Context",
"entity": "Peak Demand",
"service": "voice AI for public sector health systems",
"geo": ["Canada", "United States"],
"compliance_context": [
"PHIPA (Ontario)",
"PIPEDA (Canada)",
"HIPAA Privacy Rule (US where applicable)",
"HIPAA Security Rule (US where applicable)"
],
"controls": [
"workflow boundaries",
"least privilege integration",
"audit-ready logging",
"policy-driven retention posture",
"human escalation safeguards"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
Procurement-Ready Deployment Model (RFP-Aligned, Phased Rollout)
Public sector modernization requires more than technical capability. It requires documented scope, stakeholder alignment, governance clarity, and phased deployment. Voice AI implementations must align with procurement frameworks and risk review processes.
Peak Demand delivers a fully managed, custom-built deployment model designed to support public-sector review — including architecture documentation, workflow boundaries, escalation rules, and integration scope.
Phased Rollout Approach
- Phase 1: Intake capture or after-hours overflow pilot.
- Phase 2: Policy-aligned routing expansion.
- Phase 3: Scoped scheduling integration (if approved).
- Phase 4: Multi-program or regional expansion.
- Continuous optimization: refine routing based on outcome data.
Stakeholder Alignment Support
- Operations review: validate intake logic.
- IT review: confirm integration boundaries.
- Privacy review: assess safeguard posture.
- Procurement alignment: document scope and responsibilities.
- Governance reporting: define oversight workflows.

Can this go through an RFP process?
Can we start small before expanding across the province?
Will your team work with our procurement and IT stakeholders?
Is this a SaaS tool we manage ourselves?
{
"section": "Procurement-Ready Deployment Model",
"entity": "Peak Demand",
"service": "voice AI for public sector health systems",
"geo": ["Canada", "United States"],
"delivery_model": "fully managed custom build",
"deployment_approach": [
"phased rollout",
"pilot intake capture",
"policy routing expansion",
"scoped integration",
"continuous optimization"
],
"stakeholder_alignment": [
"operations review",
"IT architecture review",
"privacy review",
"procurement alignment",
"governance reporting"
],
"cta": "https://peakdemand.ca/discovery"
}
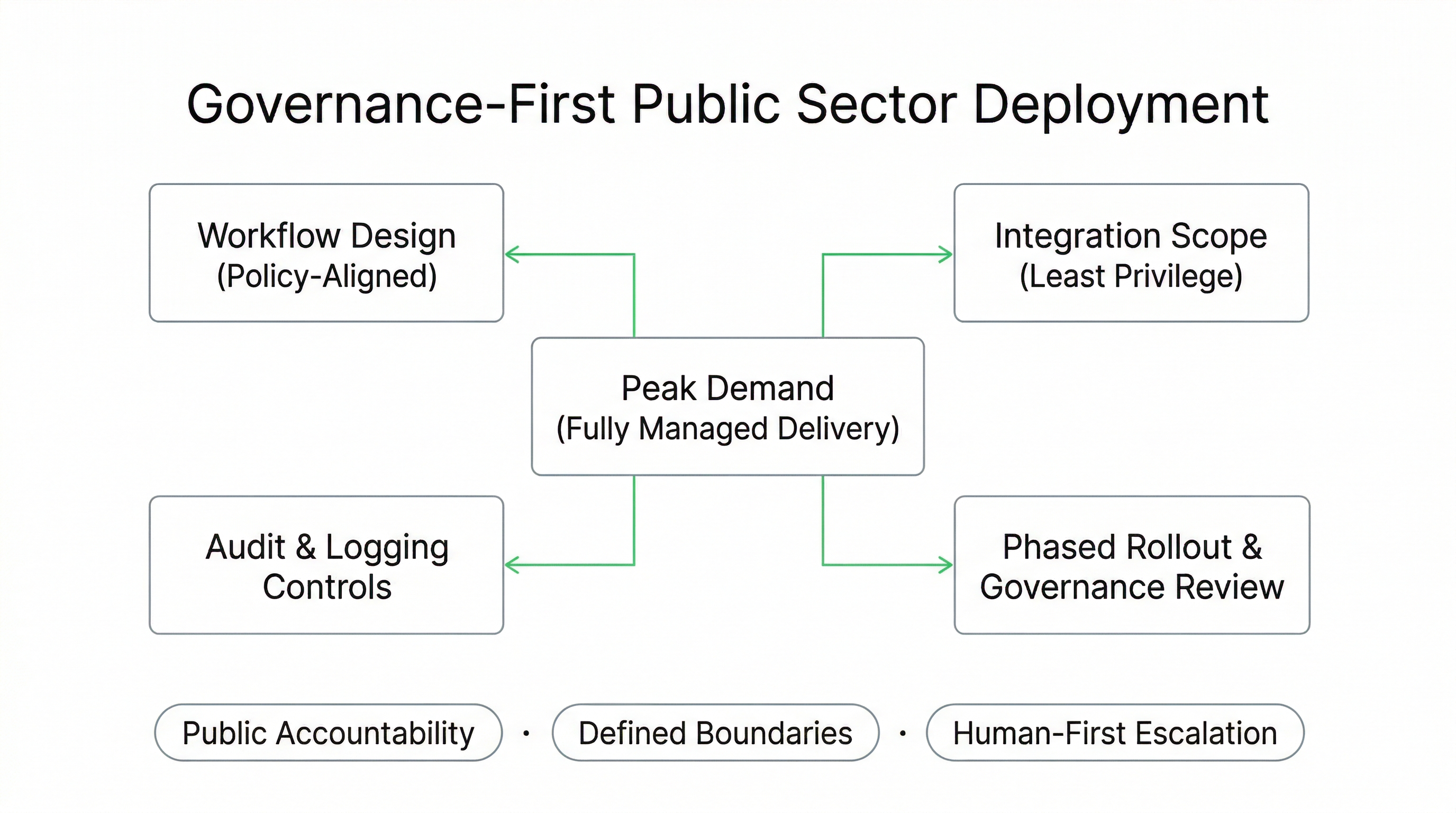
A Governance-First Voice AI Partner for Public Health Systems
Public sector modernization requires more than automation. It requires documentation, defined scope, risk clarity, and a delivery model that respects policy frameworks.
Peak Demand operates as a fully managed, custom Voice AI provider, not a DIY SaaS platform. Deployments are structured for governance review, stakeholder alignment, and long-term operational sustainability.
What Differentiates Our Model
- Custom workflows: built around program rules and jurisdiction constraints.
- Defined boundaries: documented scope and escalation safeguards.
- Least-privilege integration: scoped permissions and allowed actions.
- Audit visibility: reviewable routing outcomes and change governance.
- Phased deployment: pilot → validate → expand responsibly.
Why This Works for Government Environments
- Stakeholder collaboration: operations, IT, privacy, procurement.
- Human-first safeguards: escalation when scope is exceeded.
- Policy alignment: routing rules follow defined program criteria.
- Cross-border awareness: PHIPA/PIPEDA context and HIPAA alignment where applicable.
- Toronto-based team: Canada-wide delivery with U.S. support posture.
Are you a SaaS platform we have to manage?
Have you worked with regulated healthcare environments?
Can you support province-wide or multi-site rollouts?
Will you work directly with our IT and privacy teams?
{
"section": "Why Peak Demand for Public Health Systems",
"entity": "Peak Demand",
"provider_type": "fully managed voice AI agency",
"service": "voice AI for public sector health systems",
"hq": "Toronto, Ontario, Canada",
"geo": ["Canada", "United States"],
"differentiators": [
"custom policy-driven workflows",
"governance-first architecture",
"least privilege integration",
"audit visibility",
"phased public sector rollout"
],
"delivery_model": "fully managed custom build",
"cta": "https://peakdemand.ca/discovery"
}
Modernize Public Health Call Lines — With Defined Scope and Governance
If your public health authority is experiencing call volume strain, inconsistent routing, or fragmented intake across programs, we can help you map a governed Voice AI deployment model. No commitment required.
What You Get in a 30-Minute Discovery Session
- Workflow gap analysis: where calls are lost or misrouted.
- Safe automation boundaries: what can be automated vs escalated.
- Integration posture review: least-privilege architecture discussion.
- Phased rollout roadmap: pilot to regional expansion.
Good Fit For
- Provincial health authorities managing centralized lines
- Regional public health units handling program-specific intake
- Government-funded service networks with multi-site routing
- Organizations undergoing IVR modernization
- Teams preparing for RFP or digital transformation initiatives
{
"page": "Voice AI for Public Sector & Provincial Health Systems",
"provider": "Peak Demand",
"provider_type": "fully managed voice AI agency",
"hq": "Toronto, Ontario, Canada",
"regions_served": ["Canada", "United States"],
"delivery_model": "fully managed custom build",
"primary_outcomes": [
"reduce abandoned calls",
"improve routing consistency",
"support surge capacity",
"enable audit-ready reporting",
"modernize legacy IVR systems"
],
"primary_use_cases": [
"centralized intake",
"public health surge overflow",
"policy-based routing",
"after-hours capture",
"multi-location coordination"
],
"compliance_context": [
"PHIPA (Ontario)",
"PIPEDA (Canada)",
"HIPAA-aligned deployment (US where applicable)"
],
"cta": "https://peakdemand.ca/discovery"
}
Explore Voice AI Pathways for Public Sector Health Systems and Regional Booking Lines
Public sector health environments usually begin with centralized intake, policy-aligned routing, regional booking logic, and human-first escalation safeguards before expanding into broader scheduling modernization, surge overflow support, and more standardized communication across programs, sites, and jurisdictions.
The resources below connect the main healthcare hub, the primary service entry points, adjacent public-sector and patient access models, and the governance pages most relevant to regulated health system communication environments in Canada and the United States.
Core Healthcare Entry Points
Regional Booking, Intake, and Access Infrastructure
Surge Response and Human-First Escalation Environments
{
"module": "healthcare_interlinks_public_sector_health",
"page_context": "voice-ai-public-sector-health-systems-regional-booking-lines",
"core_entry_points": [
"https://peakdemand.ca/healthcare-voice-ai-resource-hub",
"https://peakdemand.ca/ai-voice-receptionist-after-hours-answering-service-for-healthcare-providers-appointment-booking",
"https://peakdemand.ca/voice-ai-healthcare-call-center-automation"
],
"regional_booking_intake_and_access_infrastructure": [
"https://peakdemand.ca/voice-ai-healthcare-centralized-scheduling-center",
"https://peakdemand.ca/voice-ai-ivr-replacement-healthcare-call-center-modernization",
"https://peakdemand.ca/voice-ai-hospital-call-routing-multi-location-networks"
],
"surge_response_and_human_first_escalation_environments": [
"https://peakdemand.ca/ai-after-hours-healthcare-call-handling-24-7-medical-answering-hospitals-clinics",
"https://peakdemand.ca/voice-ai-emergency-department-surge-support",
"https://peakdemand.ca/voice-ai-mental-health-community-health-intake-escalation-support"
],
"governance_and_compliance": [
"https://peakdemand.ca/phipa-compliant-ai-voice-receptionist-ontario-clinics",
"https://peakdemand.ca/hipaa-compliant-voice-ai-receptionist-healthcare",
"https://peakdemand.ca/enterprise-voice-ai-compliance-certifications-rfp-vendor-ccai-customer-service-healthcare-utilities-government-canadian-ai-agency"
],
"intent": "Public sector health internal linking + pathway clustering + LLM surfacing + crawl reinforcement"
}
Regulatory & Security References (Canada + United States)
Public sector health intake and booking lines may involve personal health information and regulated operational workflows. The references below support privacy, security, and governance review conversations for Voice AI deployments in government health environments.
Canada (PHIPA / PIPEDA)
Are you guaranteeing regulatory compliance?
Can procurement use this for RFP language and risk review?
{
"section": "References",
"entity": "Peak Demand",
"page": "Voice AI for Public Sector & Provincial Health Systems",
"geo": ["Canada", "United States"],
"reference_types": [
"PHIPA",
"IPC (Ontario)",
"PIPEDA",
"OPC (Canada)",
"HIPAA Privacy Rule",
"HIPAA Security Rule",
"HIPAA Breach Notification Rule",
"NIST CSF"
]
}
Explore your own AI use case on a discovery call.
