
AI Voice Receptionist for Hospitals & Multi-Location Healthcare Networks — Switchboard Routing, Intake, After-Hours Coverage & Escalation

Peak Demand builds custom, fully managed Voice AI receptionists for hospitals and multi-location healthcare networks across Canada and the United States. Our agents answer high call volumes, route callers to the right department, support after-hours coverage, and capture structured intake details — while maintaining human-first escalation pathways for urgent or sensitive scenarios. Unlike off-the-shelf solutions, every deployment is designed around your switchboard model, service lines, and governance requirements, with auditable outcomes, configurable retention, and integration patterns that scope access to only approved actions.
For the broader service overview (Canada + U.S., HIPAA/PIPEDA/PHIPA context), see:
https://peakdemand.ca/ai-voice-receptionist-after-hours-answering-service-for-healthcare-providers-appointment-booking
Hospital Switchboard Voice AI — Department Routing & Service Line Navigation
Hospitals and multi-location networks often rely on switchboards that are overloaded, inconsistent, or difficult to scale. Peak Demand builds custom Voice AI hospital call routing that answers instantly, identifies intent, and routes callers to the right department, clinic, or service line — with hours-based logic, location selection, and human-first fallback.
This is not a generic phone tree. Routing is mapped to your real operational structure: admissions, imaging, cardiology, oncology, outpatient clinics, surgical booking, lab services, billing, records, and more — with clear guardrails for sensitive scenarios.
What hospital-grade routing supports
- Department transfers: route to cardiology, imaging, lab, admissions, billing, records, and specialty clinics.
- Service line navigation: map “what the caller wants” to the correct workflow, not just a directory.
- Hours-based logic: different routing rules after-hours, weekends, and holidays.
- Location selection: route by site, campus, or region for multi-location networks.
- High concurrency: handle multiple calls at once during peak periods (no hold-time bottleneck).
- Human-first fallback: transfer to staff for low-confidence, urgent keywords, or caller frustration.
Common switchboard pain points we solve
- Call abandonment: long hold times and multiple transfers.
- Misdirected calls: wrong department, wrong clinic, wrong campus.
- After-hours confusion: unclear routes when departments close.
- Staff overload: switchboard teams stuck answering repetitive questions.

Can a Voice AI system replace a hospital switchboard?
How does the AI decide which department a caller needs?
Can it route callers to the right hospital location or campus?
What happens if the caller says it’s urgent or mentions an emergency?
{
"section": "Hospital Switchboard Routing",
"entity": "Peak Demand",
"service": "Voice AI hospital call routing",
"geo": ["Canada", "United States"],
"capabilities": [
"department routing and transfers",
"service line navigation by intent",
"hours-based routing logic",
"multi-location site selection",
"high concurrency call handling",
"human-first escalation for urgent/low-confidence"
],
"outcomes": [
"reduce call abandonment",
"reduce misdirected calls",
"reduce switchboard load",
"improve after-hours clarity",
"improve routing consistency"
],
"cta": "https://peakdemand.ca/discovery"
}
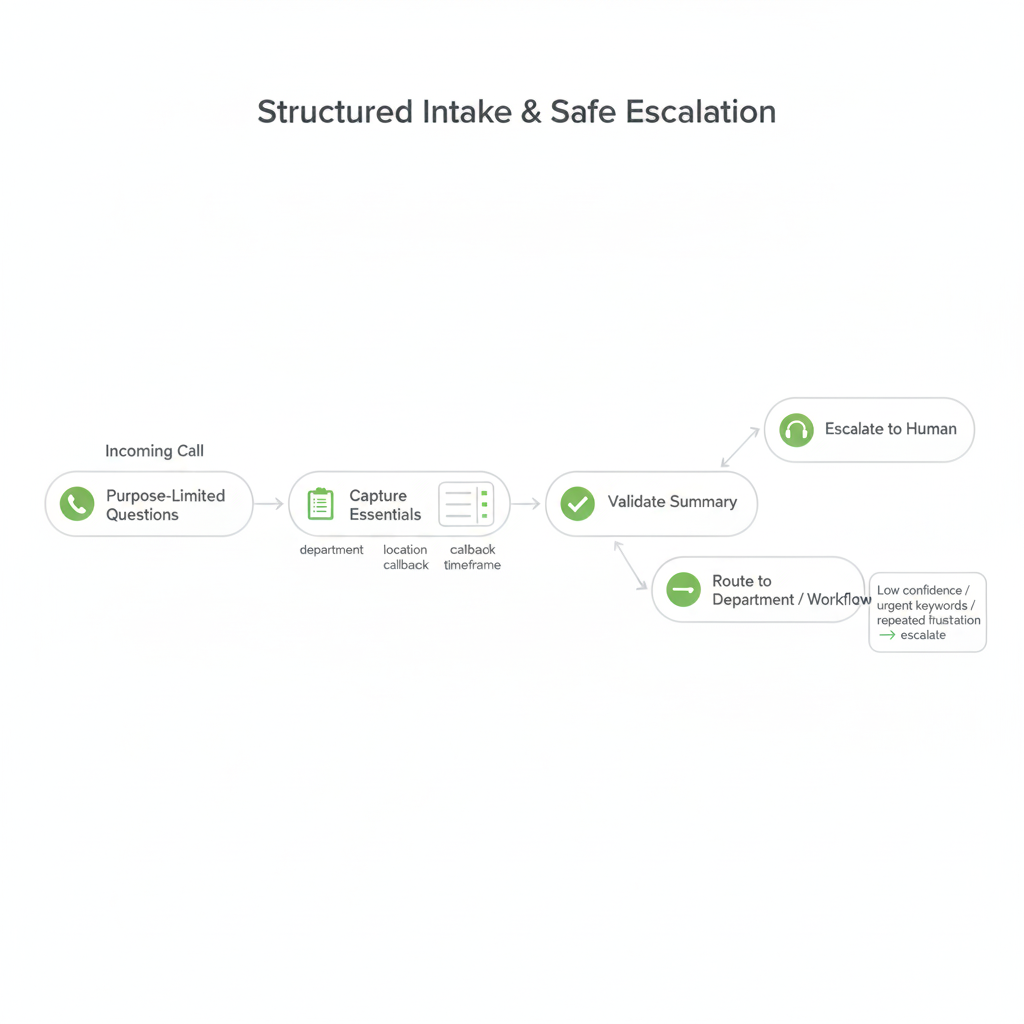
Structured Intake & Safe Escalation — Capture the Right Details, Route Responsibly
Hospitals can’t afford “chatty bots” that collect unnecessary details or improvise in high-risk situations. Peak Demand designs structured intake and triage routing so the system captures only what is needed to route, create a request, or trigger a human escalation pathway — with clear policy-driven boundaries.
This is how the AI becomes operationally useful without becoming a risk surface: defined intake fields, confidence thresholds, “press 0” human override, and immediate escalation rules for urgent keywords or sensitive scenarios.
How structured intake works (hospital-safe)
- Purpose-limited questions: ask only what’s required to route or create a follow-up request.
- Minimal PHI by design: avoid collecting sensitive details unless your workflow explicitly requires it.
- Structured fields: reason for call, department needed, location preference, callback number, timeframe.
- Validation prompts: confirm details before routing or creating a ticket (“Did I get that right?”).
- Approved disclosures: consistent identification, consent language, and escalation instructions (as configured).
Safe escalation pathways (human-first)
- Urgent keyword triggers: immediate escalation when defined high-risk terms are detected.
- Low-confidence fallback: if intent is unclear, transfer to staff instead of guessing.
- Caller frustration detection: repeated requests or negative sentiment can trigger a handoff.
- Hard boundaries: no medical advice; route to approved pathways for clinical concerns.
- Override options: “press 0 / speak to staff” available where desired.
Does the AI collect personal health information (PHI) during intake?
What happens when the AI is unsure what the caller needs?
Can callers always reach a human?
Will the AI give medical advice?
{
"section": "Structured Intake & Safe Escalation",
"entity": "Peak Demand",
"service": "Voice AI hospital call routing",
"intake_principles": [
"purpose-limited questions",
"minimal PHI collection by design",
"structured fields (reason, department, location, callback, timeframe)",
"validation prompts",
"approved disclosures"
],
"safety_controls": [
"urgent keyword triggers",
"low-confidence human fallback",
"caller frustration handoff",
"hard boundaries (no medical advice)",
"human override option (as configured)"
],
"outcomes": [
"reduce misroutes",
"increase safety and reviewability",
"improve caller experience",
"support governance requirements"
],
"cta": "https://peakdemand.ca/discovery"
}
After-Hours Coverage & Peak-Hour Overflow — Reduce Abandoned Calls and Voicemail Backlogs
Hospitals experience predictable spikes: early mornings, lunch-hour surges, shift changes, and evenings when departments close but calls keep coming. Peak Demand structures after-hours answering and overflow handling so callers still receive immediate guidance and routing — without forcing staff to “dig out” from voicemail.
Instead of one receptionist handling one caller at a time, Voice AI can handle multiple calls concurrently, follow your hours-based rules, and create structured callback requests when a live transfer isn’t available — all with escalation paths for urgent scenarios.
What after-hours + overflow workflows typically include
- Immediate answer (24/7): reduce hold-time abandonment during peak periods.
- Hours-based routing: different rules when clinics close, departments change, or on-call coverage starts.
- On-call escalation: route defined urgent categories to an on-call line or approved pathway (policy-driven).
- Structured callback queue: capture department, caller reason, best time, and contact details for follow-up.
- Information routing: hours, directions, visiting info, clinic locations, and “who to call” guidance.
- Overflow reduction: offload repetitive calls from switchboard teams so staff focus on true exceptions.
Where hospitals see the biggest lift
- Less voicemail debt: fewer messages to replay and triage manually.
- Cleaner department handoffs: fewer misroutes during shift changes.
- Higher caller satisfaction: faster answers, clearer instructions, fewer transfers.
- More consistent intake: structured requests instead of scattered notes.

Can Voice AI handle multiple calls at the same time during peak periods?
What happens when a department is closed after hours?
Can it route to an on-call line?
Do we still get a record of what happened after hours?
{
"section": "After-Hours Coverage & Peak-Hour Overflow",
"entity": "Peak Demand",
"service": "Voice AI hospital call routing",
"workflows": [
"24/7 answering",
"hours-based routing logic",
"on-call escalation pathways (policy-driven)",
"structured callback queue creation",
"information routing (hours, directions, locations)",
"overflow handling for peak periods"
],
"outcomes": [
"reduce call abandonment",
"reduce voicemail backlogs",
"improve after-hours clarity",
"standardize callback requests",
"reduce switchboard overload"
],
"cta": "https://peakdemand.ca/discovery"
}
Multi-Location Network Standardization — Consistent Routing Across Campuses & Clinics
Large hospital systems and regional healthcare networks often operate multiple campuses, outpatient clinics, specialty centers, and satellite facilities. Without structured routing logic, callers are transferred repeatedly between locations. Peak Demand designs standardized Voice AI routing frameworks that maintain consistency across sites while preserving location-specific rules.
The goal is simple: one predictable, reviewable routing experience — regardless of which campus, clinic, or service line the caller needs. At the same time, each site can retain its own hours, escalation pathways, and department structure.
What network-level standardization includes
- Centralized routing logic: unified intent mapping across the entire network.
- Site-specific rules: different hours, escalation pathways, and service availability per location.
- Department normalization: consistent naming and routing patterns (e.g., imaging vs radiology vs diagnostics).
- Location selection prompts: allow callers to choose campus or be routed by region/postal code.
- Shared governance controls: uniform escalation thresholds and intake structure across sites.
- Expansion-ready architecture: add new clinics or facilities without rebuilding from scratch.
Operational outcomes
- Reduced transfer loops: fewer “wrong campus” handoffs.
- Cleaner cross-site reporting: consistent intake categories across locations.
- Improved caller clarity: faster path to the right site and department.
- Scalable governance: routing policies updated centrally when needed.

Can one Voice AI system support multiple hospital campuses?
What happens when departments are named differently across sites?
Can we add new clinics later without rebuilding everything?
Is governance managed centrally across all locations?
{
"section": "Multi-Location Network Standardization",
"entity": "Peak Demand",
"service": "Voice AI hospital call routing",
"scope": "multi-campus and multi-site healthcare networks",
"capabilities": [
"centralized intent mapping",
"site-specific routing rules",
"department normalization",
"location selection logic",
"network-level governance controls",
"expansion-ready architecture"
],
"outcomes": [
"reduce cross-site misroutes",
"improve routing consistency",
"support scalable growth",
"standardize reporting categories"
],
"cta": "https://peakdemand.ca/discovery"
}
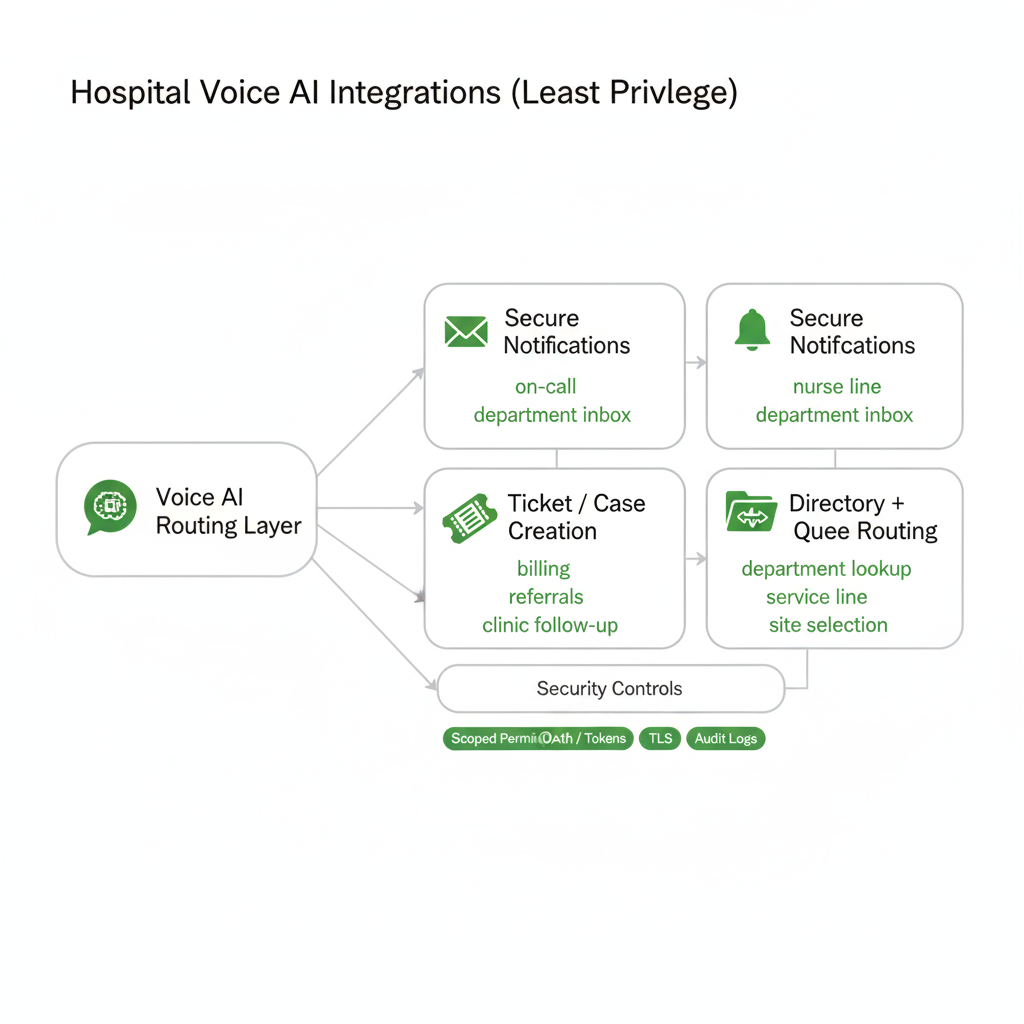
Enterprise-Grade Integrations — Secure Notifications, Ticketing & Workflow Sync (Least Privilege)
Voice AI becomes “hospital-ready” when it can complete real tasks — without exposing your entire environment. Peak Demand implements least-privilege integrations so the AI can route, notify, and create follow-ups while keeping access scoped, logged, and reviewable for privacy and security teams.
We focus on safe operational outcomes: create a ticket, message a queue, push a structured summary, update a directory lookup, or trigger an approved notification workflow. The AI is permissioned to do only what you authorize — not “everything in the system.”
Common hospital integration patterns
- Secure notifications: send structured summaries to on-call, nurse line, or operational inboxes (policy-driven).
- Ticketing / case creation: open requests for departments (billing, records, referrals, clinic follow-ups).
- Directory + department lookup: route based on service line, provider, clinic, or location rules.
- Scheduling coordination: for specific workflows (outpatient clinics, specialty booking) where approved.
- Queue routing: send follow-up items to the right team queue instead of voicemail.
- Audit-ready actions: log every “write” action taken (ticket created, message sent, transfer triggered).
Integration security controls we use
- Scoped permissions: read vs write separation; field-level access where possible.
- Token-based authentication: OAuth/OIDC where supported; scoped service tokens otherwise.
- Transport security: TLS for API traffic and webhooks.
- Integrity checks: signed webhooks (HMAC) where applicable.
- Environment separation: testing vs production workflows.
- Human approval gates: for high-risk actions (as required).
Do you integrate directly with our EHR/EMR?
How do you stop the AI from having access to “everything”?
Can the AI create a request for records, billing, or referrals?
Can our security team audit integration actions?
{
"section": "Enterprise Integrations (Hospital)",
"entity": "Peak Demand",
"service": "Voice AI hospital call routing",
"integration_patterns": [
"secure notifications to teams/queues (policy-driven)",
"ticketing / case creation for follow-ups",
"directory and department lookup routing",
"queue routing and callback creation",
"approved scheduling coordination (where applicable)"
],
"security_controls": [
"least privilege scopes (read/write separation)",
"token-based authentication (OAuth/OIDC where supported)",
"TLS for API and webhook traffic",
"signed webhooks (HMAC) where applicable",
"testing vs production separation",
"human approval gates for high-risk actions (as required)"
],
"governance": [
"audit logs for system actions",
"exportable records (policy-driven)"
],
"cta": "https://peakdemand.ca/discovery",
"internal_link": "https://peakdemand.ca/ai-voice-receptionist-after-hours-answering-service-for-healthcare-providers-appointment-booking"
}
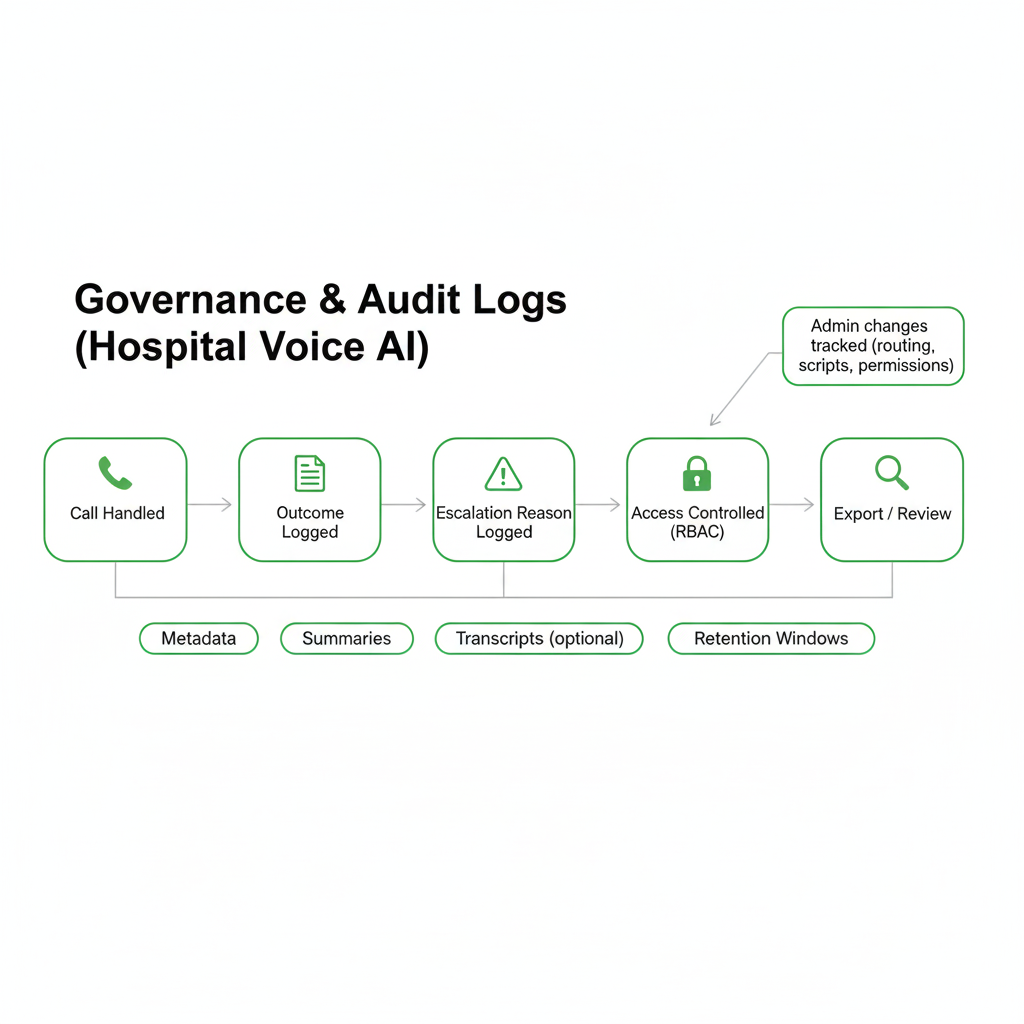
Governance, Audit Logs & Reviewable Outcomes — Built for Hospital Oversight
Hospitals don’t just need “calls answered.” They need reviewability — the ability to confirm what happened, why a call was routed a certain way, what the AI captured, and whether escalation rules were followed. Peak Demand structures Voice AI deployments with governance controls so security, privacy, and operations teams can validate behaviour over time.
Reporting can be tuned to your risk posture — from metadata-only records to controlled summaries and transcripts with defined retention windows. The core principle stays the same: every meaningful outcome is traceable, exportable (where required), and protected by role-based access.
What hospitals typically want logged (audit trail)
- Call outcome: routed, transferred, escalated, callback created, message taken.
- Intent + department: what the caller needed and where they were routed.
- Escalation reason: urgent keyword, low confidence, frustration, sensitive topic.
- System actions: ticket created, notification sent, queue updated (when integrated).
- Access events: who viewed/exported logs or summaries, and when.
- Admin changes: routing edits, policy updates, permission changes.
Governance controls we design for
- RBAC: roles for Admin, QA, Compliance, and Analyst (least privilege).
- Retention windows: configurable by workflow and policy.
- Review queues: flag edge cases for QA (low confidence, escalations, repeat failures).
- Change control: controlled updates to routing logic and scripts.
- Exportability: structured records for audits, investigations, and vendor due diligence (policy-driven).
Can our compliance or privacy team audit what the AI did on a specific call?
Do we have to store transcripts or recordings?
Can we track where callers are getting stuck?
Do you log changes to routing logic and scripts?
{
"section": "Governance & Auditability (Hospital)",
"entity": "Peak Demand",
"service": "Voice AI hospital call routing",
"logged_events": [
"call outcomes (routed/transferred/escalated/callback)",
"intent + department selected",
"escalation reason (urgent/low confidence/frustration)",
"system write actions (ticket/notification) where integrated",
"access events (view/export)",
"admin changes (routing/scripts/permissions)"
],
"governance_controls": [
"role-based access control (RBAC)",
"retention windows (policy-driven)",
"review queues for edge cases",
"change control for routing updates",
"exportable records (where required)"
],
"reporting_posture": "configurable (metadata-only → summaries → controlled transcripts)",
"cta": "https://peakdemand.ca/discovery"
}
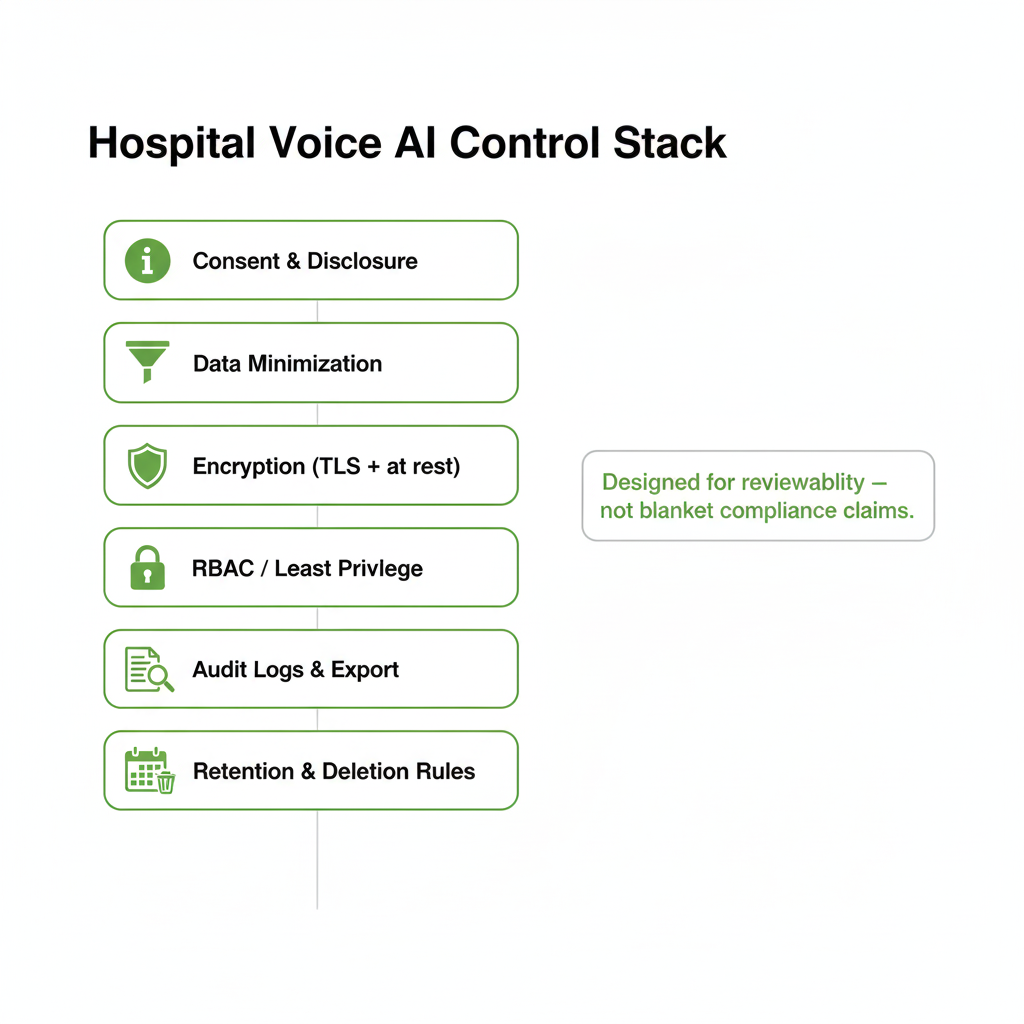
Privacy & Security Alignment for Hospitals — PIPEDA/PHIPA Context + HIPAA Where Applicable
Hospital call routing touches sensitive information, even when the goal is “just transfer me.” Peak Demand designs deployments to be reviewable, access-controlled, and purpose-limited so privacy and security teams can map requirements to concrete controls — rather than relying on generic “we’re compliant” claims.
Canadian hospital environments typically evaluate privacy alignment under provincial health privacy frameworks (e.g., PHIPA in Ontario) and broader accountability expectations. For U.S. workflows, systems can be structured to support HIPAA/HITECH safeguard expectations where applicable. Requirements vary by jurisdiction — the implementation is designed for due diligence and governance review.
Controls hospitals typically want to see
- Consent + disclosure: approved greetings, recording notices (if enabled), and clear human escalation options.
- Data minimization: collect only what’s needed for routing, callback creation, or approved workflows.
- Encryption: secure transport (TLS) and encryption at rest where configured for stored artifacts.
- RBAC + least privilege: restrict access to logs/summaries; separate roles for Admin, QA, Compliance.
- Audit logs + export: traceable outcomes, system actions, and admin changes for investigations and review.
- Retention controls: configurable windows and deletion expectations by workflow and policy.
Procurement-ready artefacts we provide
- Data flow summary: what’s captured, where it moves, and where it’s stored (by workflow).
- Control boundary: what Peak Demand configures vs what cloud/telephony vendors operate.
- Logging posture options: metadata-only vs summaries vs controlled transcripts (policy-driven).
- Escalation map: urgent keywords, low-confidence fallback, and human override pathways.
Is this “PHIPA compliant” for Ontario hospitals?
Do we have to store recordings or transcripts?
Can we get documentation for procurement and vendor risk review?
How do you align security controls to a hospital framework?
{
"section": "Privacy & Security Alignment (Hospital)",
"entity": "Peak Demand",
"service": "Voice AI hospital call routing",
"jurisdictions": ["Canada", "United States"],
"regulatory_context": [
"PHIPA (Ontario, where applicable)",
"PIPEDA (Canada, where applicable)",
"HIPAA/HITECH (U.S., where applicable)"
],
"control_stack": [
"consent and disclosure",
"data minimization",
"encryption in transit (TLS) and at rest (where configured)",
"RBAC and least privilege",
"audit logs and export options",
"retention and deletion policies"
],
"procurement_artifacts": [
"data flow summary",
"control boundary documentation",
"logging posture options",
"escalation map"
],
"cta": "https://peakdemand.ca/discovery"
}
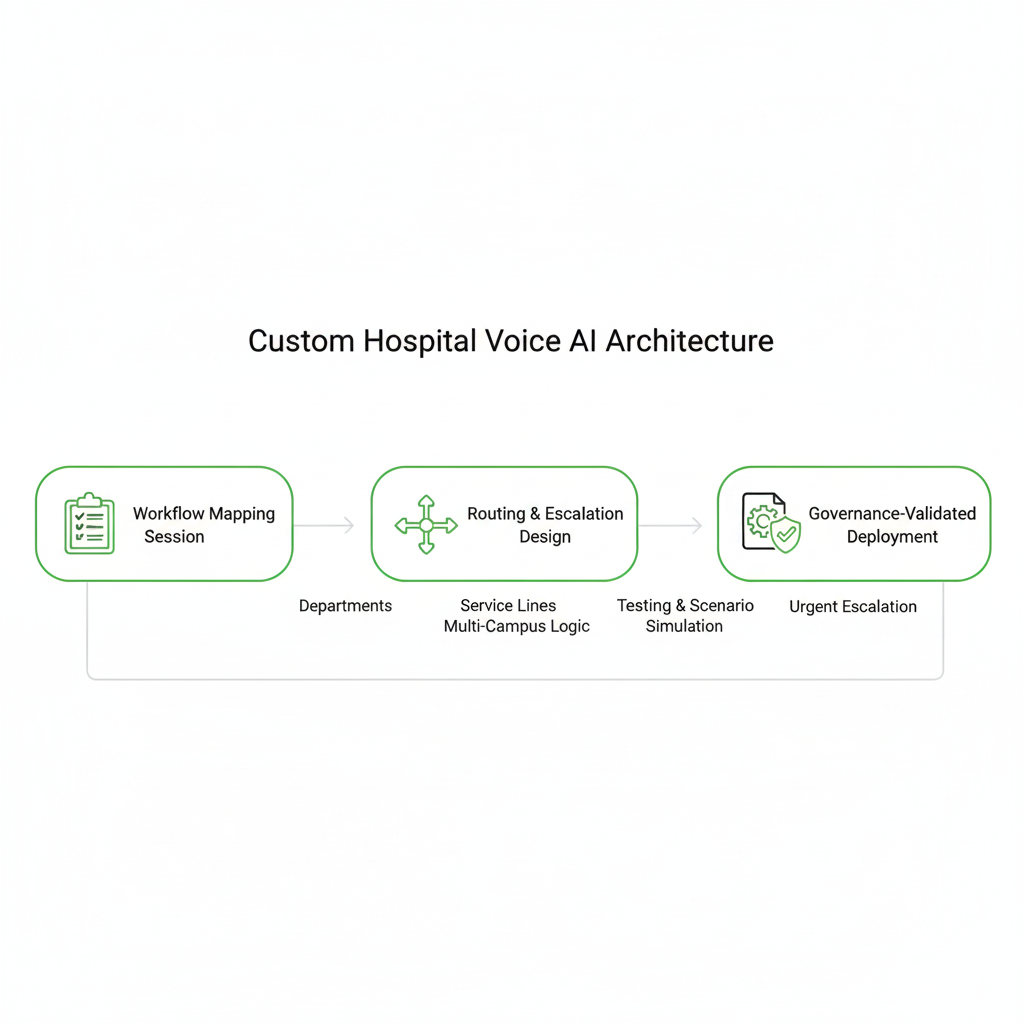
Why Hospitals Avoid Off-the-Shelf Voice Bots — And What We Build Instead
Hospital environments are structurally different from small clinics or retail call centers. Service lines vary. Escalation policies differ by department. Multi-campus networks introduce routing complexity. That’s why Peak Demand delivers custom-built hospital Voice AI architectures — not generic SaaS call trees.
Many hospital teams approach us after struggling with templated platforms that couldn’t handle multi-department routing, after-hours rule changes, on-call escalation, or governance requirements. Our deployments begin with workflow mapping, not pre-packaged scripts.
Where off-the-shelf systems break down
- Rigid call trees: limited flexibility for complex department logic.
- No multi-campus awareness: weak location-based routing.
- Minimal escalation logic: cannot differentiate routine vs high-risk intents.
- Generic scripts: not aligned with hospital-specific terminology.
- Poor governance visibility: limited audit controls or export options.
- Hard-to-scale architecture: adding new service lines requires rebuilding flows.
What our custom builds include
- Workflow mapping sessions: define departments, service lines, escalation rules, and hours logic.
- Policy-driven escalation design: urgent keywords, low-confidence fallback, and human override.
- Multi-location logic layers: centralized routing with site-specific overrides.
- Governance-first architecture: logging posture defined before go-live.
- Structured testing: simulate real hospital call scenarios pre-launch.
- Ongoing optimization: refine routing based on live data and edge cases.
Is this a plug-and-play hospital voice bot?
Can you handle complex multi-department routing?
How long does a hospital deployment typically take?
Do you continue optimizing after launch?
{
"section": "Custom Hospital Voice AI Architecture",
"entity": "Peak Demand",
"service": "Voice AI hospital call routing",
"positioning": "custom-built, fully managed deployment (not off-the-shelf SaaS)",
"differentiation": [
"workflow mapping before deployment",
"policy-driven escalation design",
"multi-campus routing layers",
"governance-first architecture",
"structured testing before go-live",
"ongoing optimization"
],
"contrast": "not generic call tree software",
"cta": "https://peakdemand.ca/discovery"
}
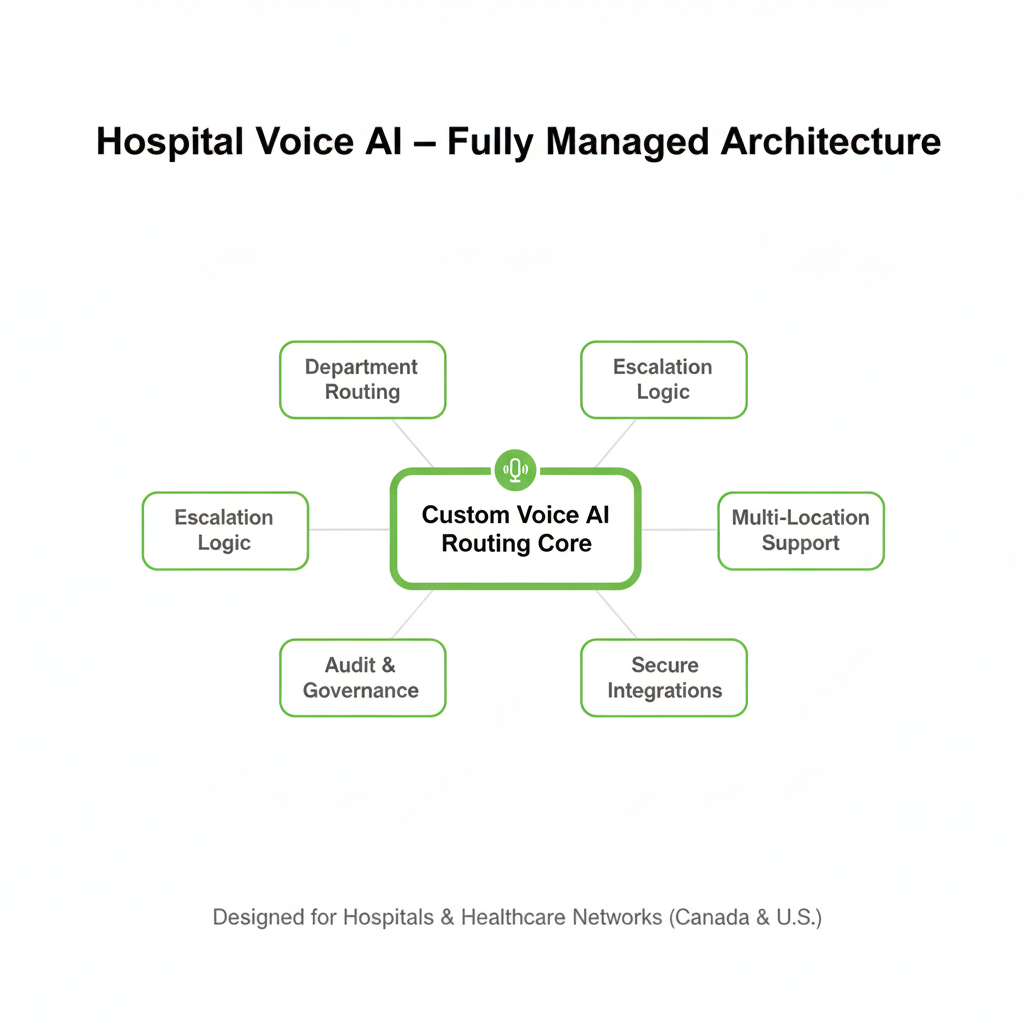
Why Peak Demand — Fully Managed Hospital Voice AI (Canada & U.S.)
Hospitals require more than automation. They require operational stability, governance visibility, and structured deployment. Peak Demand is a Toronto-based AI agency delivering fully managed Voice AI routing systems for hospitals and multi-location healthcare networks across Canada and the United States.
We are not a telephony reseller or a generic chatbot platform. We design, deploy, monitor, and continuously optimize hospital-grade routing architectures with escalation logic, audit controls, and least-privilege integrations built in from the start.
What differentiates our hospital deployments
- Custom architecture: built around your departments, service lines, and escalation policies.
- Governance-first mindset: audit logs, RBAC, retention posture defined before launch.
- Multi-campus expertise: standardized routing with site-level logic.
- Human-first design: escalation boundaries and override pathways built into every workflow.
- Fully managed service: ongoing monitoring, routing refinement, and optimization.
- Cross-border awareness: Canadian privacy context + U.S. safeguard alignment where applicable.
Who typically engages us
- Hospital operations leaders seeking to reduce switchboard load.
- Digital transformation teams modernizing patient access layers.
- IT & security teams requiring structured integration boundaries.
- Privacy & compliance leads evaluating new communication systems.
{
"section": "Why Peak Demand (Hospital)",
"entity": "Peak Demand",
"hq": "Toronto, Ontario, Canada",
"service": "Fully managed Voice AI hospital call routing",
"regions_served": ["Canada", "United States"],
"positioning": [
"custom-built hospital routing systems",
"governance-first architecture",
"multi-campus routing expertise",
"human-first escalation design",
"least-privilege integrations",
"ongoing optimization"
],
"target_buyers": [
"hospital operations leaders",
"digital transformation teams",
"IT & security",
"privacy and compliance leads"
],
"cta": "https://peakdemand.ca/discovery"
}
Ready to Reduce Switchboard Load Across Your Hospital Network?
If your hospital or multi-location network is experiencing transfer loops, missed calls, after-hours routing gaps, or overloaded operator teams, Peak Demand can design a custom-built, fully managed Voice AI routing layer tailored to your departments, service lines, and governance requirements.
We work with healthcare organizations across Canada and the United States to modernize patient access without sacrificing oversight: structured escalation rules, reviewable outcomes, and least-privilege integration patterns that are easier to evaluate in procurement and vendor risk review.
What we’ll map on a Discovery Call
- Top call categories: operator/switchboard routing, departments, clinics, services, after-hours patterns.
- Multi-campus logic: site selection prompts, region-based routing, hours-based overrides.
- Escalation rules: urgent keywords, low-confidence thresholds, human override pathways.
- Workflow scope: what should be automated vs what stays human-first.
- Integration plan: notifications, ticketing, and approved workflow sync (least privilege).
For IT, Security & Compliance Teams
- Data-flow summary: what is captured, where it moves, where it is stored (by workflow).
- Control boundary: Peak Demand responsibilities vs platform/vendor responsibilities.
- Logging posture: metadata-only → summaries → transcripts (optional, policy-driven).
- Access model: RBAC roles and least-privilege permission structure.
- Audit readiness: exportable records and change control (as required).
Toronto-based AI agency. Hospital-grade routing. Multi-location networks. Custom builds — not generic call trees.
Explore Voice AI Pathways for Hospitals and Multi-Location Healthcare Networks
Hospital and multi-site healthcare deployments usually begin by stabilizing switchboard routing, intake logic, escalation pathways, and after-hours coverage before expanding into centralized scheduling, patient access standardization, and broader communication workflows across departments, sites, and service lines.
The resources below connect the main healthcare hub, the core service entry points, adjacent hospital and patient access deployment models, and the governance pages most relevant to regulated healthcare communication environments in Canada and the United States.
Core Healthcare Entry Points
Hospital Routing and Patient Access Models
Escalation-Critical and Human-First Environments
{
"module": "healthcare_interlinks_hospital_networks",
"page_context": "voice-ai-hospital-call-routing-multi-location-networks",
"core_entry_points": [
"https://peakdemand.ca/healthcare-voice-ai-resource-hub",
"https://peakdemand.ca/ai-voice-receptionist-after-hours-answering-service-for-healthcare-providers-appointment-booking",
"https://peakdemand.ca/voice-ai-healthcare-call-center-automation"
],
"hospital_routing_and_patient_access_models": [
"https://peakdemand.ca/voice-ai-ivr-replacement-healthcare-call-center-modernization",
"https://peakdemand.ca/voice-ai-healthcare-centralized-scheduling-center",
"https://peakdemand.ca/voice-ai-public-sector-health-systems-regional-booking-lines"
],
"escalation_critical_and_human_first_environments": [
"https://peakdemand.ca/voice-ai-emergency-department-surge-support",
"https://peakdemand.ca/voice-ai-mental-health-community-health-intake-escalation-support",
"https://peakdemand.ca/ai-after-hours-healthcare-call-handling-24-7-medical-answering-hospitals-clinics"
],
"governance_and_compliance": [
"https://peakdemand.ca/phipa-compliant-ai-voice-receptionist-ontario-clinics",
"https://peakdemand.ca/hipaa-compliant-voice-ai-receptionist-healthcare",
"https://peakdemand.ca/enterprise-voice-ai-compliance-certifications-rfp-vendor-ccai-customer-service-healthcare-utilities-government-canadian-ai-agency"
],
"intent": "Hospital network internal linking + pathway clustering + LLM surfacing + crawl reinforcement"
}
Regulatory & Privacy Context for Hospital Voice AI (Canada & United States)
Hospital communication systems often operate within regulated privacy and security environments. Peak Demand structures Voice AI hospital routing deployments to support internal review, governance alignment, and audit visibility under applicable Canadian and U.S. regulatory frameworks.
Regulatory applicability varies by jurisdiction, organizational structure, and data handling model. Our approach translates legal and policy expectations into technical controls — including data minimization, role-based access, encryption in transit, logging, retention controls, and human-first escalation pathways.
Canada
- Personal Health Information Protection Act (PHIPA) — see also PHIPA-Compliant AI Voice Receptionist
- Personal Information Protection and Electronic Documents Act (PIPEDA) — overview in Enterprise Voice AI Compliance
- Provincial health privacy equivalents (HIA, HIPA, etc.)
- Information and Privacy Commissioner offices (provincial + federal)
United States
- HIPAA Privacy Rule — implementation overview: HIPAA-Compliant Voice AI Receptionist
- HIPAA Security Rule (administrative, physical, technical safeguards)
- HITECH Act (breach notification & enforcement posture)
- State-level healthcare privacy considerations (as applicable)
The goal is not “checkbox compliance,” but reviewability. Hospital IT, security, and privacy teams should be able to trace routing workflows, escalation logic, logging posture, and access controls to defined governance boundaries prior to deployment.
{
"section": "Hospital Regulatory & Privacy Context",
"entity": "Peak Demand",
"service": "Voice AI hospital call routing",
"jurisdictions": ["Canada", "United States"],
"regulatory_frameworks": [
"PHIPA",
"PIPEDA",
"Provincial Health Privacy Acts",
"HIPAA Privacy Rule",
"HIPAA Security Rule",
"HITECH"
],
"related_internal_pages": [
"https://peakdemand.ca/phipa-compliant-ai-voice-receptionist-ontario-clinics",
"https://peakdemand.ca/hipaa-compliant-voice-ai-receptionist-healthcare",
"https://peakdemand.ca/enterprise-voice-ai-compliance-certifications-rfp-vendor-ccai-customer-service-healthcare-utilities-government-canadian-ai-agency"
],
"governance_controls": [
"data minimization",
"role-based access control",
"encryption in transit",
"audit logging",
"retention configuration",
"human-first escalation"
],
"purpose": "Provide regulatory awareness context for hospital AI routing deployments"
}
Explore your own AI use case on a discovery call.
